
(2003; Updated 2008)
{kind=link}
Out-of-Body Discrepancies
Veridical Paranormal Perception During OBEs?
Maria’s Shoe
Pam Reynolds
NDEs in the Blind?
NDE Target Identification Experiments
Psychophysiological Correlates
What are Out-of-Body Experiences?
Bodily Sensations
Living Persons
Cultural Differences
How Consistent are NDE Features across Cultures?
Random Memories
Is the Temporal Lobe Implicated in NDEs?
Threshold Crossings: Returns from the Point of No Return
Who Makes the Decision to Return?
Hallucinatory Imagery
Unfulfilled Predictions: Psychic Inability
Conclusion
Even if we disregard the overwhelming evidence for the dependence of consciousness on the brain, there remains strong evidence from reports of near-death experiences themselves that NDEs are not glimpses of an afterlife. This evidence includes:
(1) discrepancies between what is seen in the out-of-body component of an NDE and what’s actually happening in the physical world;
(2) bodily sensations incorporated into the NDE, either as they are or experienced as NDE imagery;
(3) encountering living persons during NDEs;
(4) the greater variety of differences than similarities between different NDEs, where specific details of NDEs generally conform to cultural expectation;
(5) the typical randomness or insignificance of the memories retrieved during those few NDEs that include a life review;
(6) NDEs where the experiencer makes a decision not to return to life by crossing a barrier or threshold viewed as a ‘point of no return,’ but is restored to life anyway;
(7) hallucinatory imagery in NDEs, including encounters with mythological creatures and fictional characters; and
(8) the failure of predictions in those instances in which experiencers report seeing future events during NDEs or gaining psychic abilities after them.
Out-of-Body Discrepancies
(1) Some NDErs report out-of-body experiences during their NDEs where what is seen ‘out-of-body’ does not correspond to what is actually happening in the physical world. Peter and Elizabeth Fenwick reports the NDE of a World War II veteran whose unit came under attack from aerial bombers:
The battery cook (a devout Muslim) came running in panic toward me…. He lay down, touching my right elbow, and calmed himself…. As I looked up one of the Heinkel pilots executed a tight turn over the rim of the wadi and lined up on us…. I flattened out like a lizard on the sand….
Instantly I was enveloped in a cloud of beautiful purple light and a mighty roaring sound…. and then I was floating, as if in a flying dream, and watching my body, some dozen feet below, lifting off the sand and flopping back, face downwards. I only saw my own body. I was quite unaware of the two Sudanese lying beside me…. And then I was gliding horizontally in a tunnel … rather like a giant, round, luminous culvert, constructed of translucent silken material, and at the end of a circle of bright, pale primrose light. I was enjoying the sensation of weightless, painless flight…. I had a feeling it would be more interesting when I reached the light….
I became aware that I was being ‘sucked’ back through the tunnel and then into a body that felt rather unpleasantly ‘heavy,’ that the sun was burning my back…. [T]he Heinkels were still firing at us and a cannon shell knocked a saucepan off the truck above my head. This troubled me not at all; indeed I seemed to have lost all sense of fear, but my back felt wet and slimy so I looked over my shoulder to investigate the cause. My back was a red mass of blood and raw flesh…. Then I realised that I was looking at all that remained of Osman the cook, who had been lying beside me. I noticed also that my Bren gunner, who had been close to my other side, had disappeared (Fenwick and Fenwick 43-44).
The Fenwicks concede that in this case it is “quite clear” that this NDEr was not actually observing the physical world when he saw his body from above. Obviously this NDE must have been a brain-generated hallucination. Despite their sympathy for the survival hypothesis, the Fenwicks are explicit about the hallucinatory nature of this NDE: “He was unaware of the cook, who had been lying beside him—and was now not simply lying beside him but spread all over his back, where he could hardly have failed to be seen” (Fenwick and Fenwick 44).[1]
(2) The Fenwicks also mention the case of a woman who had 3 spontaneous out-of-body experiences during her second pregnancy (Fenwick and Fenwick 40-41). In her third OBE, she found it difficult to ‘return to her body.’ The Fenwicks write: “Mrs Davey adds that although she was up on the ceiling, she did not see her body” (Fenwick and Fenwick 41).[2]
(3) In a case from “the Evergreen Study” (conducted at Evergreen State College in Washington), a woman had a ruptured Fallopian tube due to an ectopic pregnancy (where a fertilized egg implants and grows in one of the tubes rather than the uterus) and reported seeing things in the room while ‘out-of-body’ which didn’t exist:
I saw this little table over the operating table. You know, those little round trays like in a dental office where they have their instruments and all? I saw a little tray like that with a letter on it addressed (from a relative by marriage she had not met) (Lindley, Bryan, and Conley 109).
The authors report that this woman told her sister-in-law about her NDE, who happened to be a nurse who was called into the operating room at the time of the NDE. But the nurse was adamant that there was neither a letter nor a round table in the operating room.
However, the authors note that there was a small rectangular table for holding instruments in the room called a ‘Mayo’ and quickly deduce a probable scenario for why this experience took the form it did: “Notice [Mayo] sounds like ‘mail.’ She may have heard someone call the tray by name (since hearing is reportedly the final sense to fail at death) and connected it with ‘mail.'” (109). Moreover, the letter seen out-of-body was addressed from the nurse’s brother-in-law, which suggests that she might have heard the nurse’s name and incorporated that information into her experience as well.
What is particularly interesting about this case is not simply that it contains discrepancies, but also that it seems to confirm that out-of-body imagery in NDEs is sometimes obtained directly from scraps of conversation rather than from some paranormal source.
(4) In a study of 264 subjects with sleep paralysis[3], Giorgio Buzzi and Fabio Cirignotta found that about 11% of their subjects (28 people) “viewed themselves lying on the bed, generally from a location above the bed” (Buzzi 2116). As Buzzi points out, however, these out-of-body experiences often included false perceptions of the physical environment:
I invited these people to do the following simple reality tests: trying to identify objects put in unusual places; checking the time on the clock; and focusing on a detail of the scene, and comparing it with reality.
I received a feedback [sic] from five individuals. Objects put in unusual places (eg, on top of the wardrobe) were never identified during out-of-body experiences. Clocks also proved to be unreliable: a woman with nightly episodes of sleep paralysis had two out-of-body experiences in the same night, and for each the clock indicated an impossible time…. Finally, in all cases but one, some slight but important differences in the details were noted: “I looked at ‘me’ sleeping peacefully in the bed while I wandered about. Trouble is the ‘me’ in the bed was wearing long johns … I have never worn such a thing” (Buzzi 2116-2117).
Buzzi concludes that because these experiences contained out-of-body discrepancies and failed his other ‘reality tests,’ his subjects’ out-of-body imagery must have been derived from memory and imagination rather than from the physical environment at the time (2117).
(5) Melvin Morse reports an NDE where a young girl sees her teacher by her body during an OBE when her teacher is not actually there. This case also has other hallucinatory features, such as encountering doctors in an ostensibly transcendental realm:
[O]ne child…. could see her own body as doctors wearing green masks tried to start an IV. Then she saw her living teacher and classmates at her bedside, comforting her and singing to her (her teacher did not visit her in the hospital). Finally, three tall beings dressed in white that she identified as doctors asked her to push a button on a box at her bedside, telling her that if she pressed the green button she could go with them, but she would never see her family again. She pressed the red button and regained consciousness (Morse 68-69).
(6) Using open-ended questions, Morse also found a case where a child that was clinically dead reported that while she was ‘above her body’ looking down, “her mother’s nose appeared flattened and distorted ‘like a pig monster'” (Morse 67).
(7) The Fenwicks recount an NDE where the NDEr ‘observed’ a procedure that never took place during the heart bypass operation she underwent at the time:
[S]he left her body and watched her heart lying beside her body, bumping away with what looked like ribbons coming from it to hands. In fact, this is not what happens in a heart bypass operation, as the heart is left within the chest and is never taken outside the body (Fenwick and Fenwick 193).
The Fenwicks try to explain away this major discrepancy by pointing out that ribbons are indeed tied to arteries during an operation of this sort and by attributing the false perception to misidentification. However, it is difficult to see how a person truly out-of-body with vivid perceptual capabilities could confuse arteries (ribboned or not) with a beating heart lying next to her outside of her body. In the remainder of her experience this NDEr reported ‘traveling’ to a place that looked like an enormous silver ‘airplane hangar’ with tiny figures off in the distance, miles away.
(8) Other NDErs have reported seeing friends out-of-body with them who are, in reality, still alive and normally conscious. The Evergreen Study also recorded a clearly hallucinatory near-death experience after a major car accident:
Well, then I remember, not physical bodies but like holding hands, the two of us, up above the trees. It was a cloudy day, a little bit of clouds. And thinking here we go, we’re going off into eternity… and then bingo, I snapped my eyes open and I looked over and he was staring at me [ellipsis original] (Lindley, Bryan, and Conley 110).
The authors of the study go on to write: “In this incident a woman had lost consciousness but her male companion had not. In the experience, she perceived the two of them in an out-of-body state, yet her friend never blacked out” (110).
(9) OBErs who do not lose consciousness before their experiences often report watching their bodies continue to perform coordinated actions—as if they were still in control of their bodies—while nevertheless apparently viewing them from above. Recalling an OBE while on patrol for the first time, chasing an armed suspect, a police officer reported:
I promptly went out of my body and up into the air maybe 20 feet above the scene. I remained there, extremely calm, while I watched the entire procedure—including watching myself do exactly what I had been trained to do (Alvarado 183).
After the suspect had been restrained and the danger was over, the officer returned to normal consciousness. Another OBEr, who had been running for over 12 miles training for a marathon, reported:
I felt as if something was leaving my body, and although I was still running along looking at the scenery, I was looking at myself running as well (184).
This ability to simultaneously ‘hover’ above the scene and continue to function as if ‘in’ the body strongly suggests the hallucinatory nature of these experiences. In some sleep disorders, for instance, subjects are able to exhibit “directed” behavior—e.g., sleepwalking and sleep eating—even though they are evidently not normally conscious. Taking on an extraordinary new perspective while functioning normally otherwise makes much more sense if such experiences are occurring ‘in’ the body all along, rather than in some remote discarnate entity detached from the physical body.
(10) Finally, Harvey Irwin notes other intriguing examples of hallucinatory OBEs, such as reports of “seeing the physical body as if from a height of 30 feet (9 meters) or more … [when] this would have entailed seeing through the roof and the ceiling of the house” (Irwin, “Introduction” 223). If something leaves the body and perceives the physical world during OBEs, he asked, “why do some OBErs report distortions in reality (e.g., [nonexistent] bars on the bedroom window), and how are some experients able to manipulate the nature and existence of objects in the out-of-body environment by an effort of will?” (233).
As the Fenwicks point out, if OBEs and NDEs are hallucinations,
we should expect there to be major discrepancies between the psychological image—what the person sees from up there on the ceiling, which will be constructed by the brain entirely from memory; and the real image—what is actually going on at ground level. Mrs Ivy Davey, for example, did not see her body, although her body was clearly there (Fenwick and Fenwick 41).
And in the cases above this is exactly what we find. Discrepancies between what’s seen out-of-body and what’s actually happening in the physical world are found in spontaneous OBEs, in NDEs where a real or perceived threat of imminent harm triggers an OBE, and in NDEs that include an OBE along with other NDE components (e.g., a tunnel and light).
Veridical Paranormal Perception During OBEs?
The cases cited in this essay show that many near-death experiences are hallucinations.[4] NDE cases which include false descriptions of the physical environment have been found not only by different near-death researchers, but by researchers searching for evidence that NDEs are not hallucinatory. This motivation among researchers makes it impossible to estimate the prevalence of NDEs with clearly hallucinatory features. As Bruce Greyson points out, the file-drawer problem is a likely factor here: NDE accounts with clearly hallucinatory features may end up filed away indefinitely, while only more dramatic accounts are deemed fit for publication by NDE researchers (Greyson, “Near-Death” 344). Similarly, NDEs with obviously hallucinatory traits seem particularly likely to be underreported by NDErs themselves, given the disparity between how real one’s NDE felt at the time and the realization that it could not possibly reflect reality if, for instance, the NDEr communicated with his still-living mother in an ostensibly transcendental realm. Nevertheless, given that many NDEs are already known to be hallucinations, it is likely that other NDEs are hallucinations as well.
The majority of near-death researchers are interested in the subject because they believe NDEs provide evidence for life after death. Thus near-death researchers generally disregard hallucinatory NDEs while searching for cases of veridical paranormal perception. But at the end of the day, we are left with no compelling evidence that NDErs have actually been able to obtain information from remote locations, and we have clear evidence that NDErs sometimes have false perceptions of the physical world during their experiences.
Mark Fox provides a very balanced assessment of the evidential value of near-death experiences in his recently published Religion, Spirituality and the Near-Death Experience. As a research committee member of the Religious Experience Research Centre at the University of Wales, Lampeter, Fox is certainly no enemy of dualism. Yet he concludes that NDE research to date largely presupposes some sort of dualism rather than providing evidence for it:
This needs to be spelled out loudly and clearly: twenty-five years after the coining of the actual phrase ‘near-death experience,’ it remains to be established beyond doubt that during such an experience anything actually leaves the body. To date, and claims to the contrary notwithstanding, no researcher has provided evidence for such an assertion of an acceptable standard which would put the matter beyond doubt (Fox 340).
In fact, very few cases of ‘veridical perception’ during NDEs have been corroborated. In many cases, details which are said to have been accurate “are not the kind that can easily be checked later” (Blackmore, “Dying” 114). Even the ‘founding father’ of near-death studies, Raymond Moody, concedes that most cases of alleged veridical perception during NDEs are found well after the fact and are usually attested to only by the NDEr and perhaps a few friends (114). And in one study Carlos Alvarado found that although nearly one-fifth of participants claimed to have made “verifiable observations” during their OBEs, only 3 of the 61 cases even “qualified as potentially veridical when experients were asked to provide fuller descriptions” (Alvarado 187).
Susan Blackmore and Tillman Rodabough consider at length how accurate information can be incorporated into realistic out-of-body imagery during NDEs. Both conclude that the primary source of information in the construction of out-of-body imagery is probably hearing. Rodabough notes that patients who appear to be unconscious often repeat earlier comments made by doctors and nurses even without an OBE, and “have even been able to recall operating room conversations under hypnosis” (Rodabough 108). But Blackmore points out that other sensory sources of information are also available to patients. She notes that a residual sense of touch during NDEs could explain accurate details about where defibrillator pads were placed or where chest injections were administered (Blackmore, “Dying” 125).
Remaining out-of-body imagery is probably derived from imagination and general background knowledge. For example, Rodabough points out that childhood socialization trains us to imagine how we appear to others ‘from the outside’; thus visualizing oneself from a third-person perspective comes naturally (Rodabough 108). Blackmore notes that when people are asked to imagine walking down a beach, they usually picture themselves from above, from a bird’s-eye perspective (Blackmore, “Dying” 177). Carol Zaleski suggests that we should expect some NDEs to include OBEs because the most natural way to imagine experiencing one’s death is to imagine looking down on one’s body from above (as people typically do when asked to imagine viewing their own burials). In her lesser-known 1996 book on NDEs, The Life of the World to Come, Zaleski notes:
The people who testify to near-death experience are neither Platonists nor Cartesians, yet they find it natural to speak of leaving their bodies in this way. There simply is no other way for the imagination to dramatize the experience of death: the soul quits the body and yet continues to have a form (Zaleski, “Life” 62-63).
Background knowledge also surely plays a role. Personal experience and media portrayals make it easy for us to imagine what a hospital scene should look like (Rodabough 109). Even specific details about people are fairly predictable in a hospital setting:
When either a person or their roles [sic] is well known, it is not difficult to predict dress or behavior. For example, isn’t it easy to guess that a physician will wear his greens in surgery?[5]… Behavior, particularly where strong emotions are concerned, may be even easier to predict. Mother falls apart and begins to sob hysterically while Dad puts his arms around her in consolation and stoically keeps his anxiety inside…. [Thus] the probability of an accurate description can be high even without an out-of-body experience [emphasis mine] (Rodabough 109).
Blackmore ultimately concludes that “prior knowledge, fantasy and lucky guesses and the remaining operating senses of hearing and touch,” plus “the way memory works to recall accurate items and forget the wrong ones” is sufficient to explain out-of-body imagery in NDEs (Blackmore, “Dying” 115). Cases incorporating out-of-body discrepancies, including those based on misinterpretations of scraps of conversation (e.g., seeing mail in out-of-body imagery when ‘Mayo’ is spoken), appear to confirm this suggestion.
Our memories are constantly reconstructed as we retell stories about our pasts. When a person has an extraordinary story to tell, such as how he found himself out of his body, with all that suggests about the possibility of life after death, the likelihood of exaggeration—even unintentional exaggeration—is obvious. In such cases, ultimately “the version we tell is likely to be just that little bit more interesting or poignant than it might have been” (115).
In fact, most NDE reports are provided to researchers years after the experience itself. Ultimately, all we have to go on is after-the-fact reports of private experiences. The constant reconstruction of memory makes it difficult to know just what NDErs have actually experienced. This problem is clearly recognized by Fox:
[T]he fact that NDErs’ testimonies are indeed retrospectively composed … arouses a suspicion that what NDErs recall—and hence narrate—about their experiences may in fact be different than what they actually experienced during their near-death crises…. [A]ttempting to ascertain what really happens to NDErs—what the core elements of their experiences actually are in and of themselves—may be nigh on impossible to determine…. [W]hat is remembered about an experience or situation may not actually accurately correspond to what was experienced at the time (Fox 197).
Following Zaleski, Fox also wonders to what extent people other than the NDEr play a part in composing an NDE report. Both note, for example, Raymond Moody’s concession that he sometimes used leading questions when interviewing respondents for his 1975 Life After Life (Zaleski, “Otherworldly” 149; Fox 199). Zaleski also points out that after urging his respondents to speak freely, Kenneth Ring would ask specific questions about whether his subjects encountered features of Moody’s model of the NDE, such as: “[W]ere you ever aware of seeing your physical body?” or “Did you at any time experience a light, glow, or illumination?” (Zaleski, “Otherworldly” 105-106). After Sabom allowed his patients to speak freely, he would also “delve for the elements described in Life After Life” (Zaleski, “Otherworldly” 109). One wonders how much similarity would have been found between individual NDE accounts in the West had these early researchers simply asked their respondents to speak freely about their experiences without steering them in a particular direction by probing for Moody’s elements.
This raises further questions about the extent to which other near-death researchers have also used leading interviewing techniques (Fox 199-200). As Greyson points out, how a counselor responds to an NDEr “can have a tremendous influence on whether the NDE is accepted and becomes a stimulus for psychospiritual growth or whether it is regarded as a bizarre experience that must not be shared” [emphasis mine] (Greyson, “Near-Death” 328). While some counselors might take a dismissive attitude to such experiences, many are likely to influence NDErs in the opposite direction, and near-death researchers seem particularly likely to positively reinforce an afterlife interpretation of NDEs. This may be one reason why so many NDErs accept that interpretation. Another may be that widespread belief in an afterlife among the general population has already primed NDErs to interpret unusual experiences on the brink of death in terms of an afterlife. And on top of such outside influences, Fox notes:
[Simply] having an experience which may appear to the subject to point to the possibility of immortality—such as an OBE whilst resting or sleeping, leading to the conviction that the soul can function independently of the body—may suffice to instil in him or her an often strong and permanent belief that personal death is not the end…. And often their experiences are so vivid as to provide, for them, a solid basis for drawing conclusions across a wide range of important, existential issues: including the question of their own immortality and its relationship to the way they live and understand their lives before their deaths (Fox 287).
Taking an afterlife interpretation largely explains the transformative effects of NDEs on those who have them as well. (Though to gauge the extent of this, it would be interesting to see if “nonbelievers” had the same transformations as “survivalists” among NDErs.)[6]
Rodabough explains how unintentional interviewer feedback can contaminate NDE reports:
[I]f the resuscitated person gives a partially accurate account of some event taking place while he was “out,” the questioner may unintentionally give information which the resuscitated person unknowingly fits into his story. To some degree, we can visualize what we are told and not be sure which occurred first…. This is likely to occur if the questioner wants to hear things a particular way and nonverbally reinforces the respondent when he hears what he wants. The high enthusiasm of the interviewer may unwittingly entice the respondents to embellish their experiences, and low enthusiasm may influence respondents to remain silent about puzzling or unusual experiences (Rodabough 109-110).
In fact, in recent years a large number of NDE reports have been garnered from NDE support groups. Support group members have almost certainly shaped the content of individual NDE accounts through “biographical reshaping, deepening of commitment, and reinforcement of group belief” (Fox 201).
In The Truth in the Light, the Fenwicks asks how an experience as coherent as an NDE could be generated in a disorganized dying brain, and how it could be encoded for vivid recall later:
How is it that this coherent, highly structured experience sometimes occurs during unconsciousness, when it is impossible to postulate an organized sequence of events in a disordered brain? One is forced to the conclusion that either science is missing a fundamental link which would explain how organized experiences can arise in a disorganized brain, or that some forms of experience are transpersonal—that is, they depend on a mind which is not inextricably bound up with the brain (Fenwick and Fenwick 235).[7]
But as Gerald Woerlee points out, lack of oxygen to the brain blunts a subject’s judgment, creating a false confidence in one’s abilities and a false sense that one’s thinking is particularly keen—a well-known fact exhibited in the statements of clearly impaired drunk drivers. “This,” he argues, “is why people recovering from cardiac resuscitation never say their mental state during a period of consciousness such as an NDE was confused or befuddled” (Woerlee, “Cardiac” 246).
Greyson offers a related argument:
[O]rganic brain malfunctions generally produce clouded thinking, irritability, fear, belligerence, and idiosyncratic visions, quite unlike the exceptionally clear thinking, peacefulness, calmness, and predictable content that typifies the NDE. Visions in patients with delirium are generally of living persons, whereas those of patients with a clear sensorium as they approached death are almost invariably of deceased persons [emphasis mine] (Greyson, “Near-Death” 334).
But as we see in the case of G-LOC dreamlets (pleasurable experiences caused by lack of oxygen to the brain during pilot blackouts), some “organic brain malfunctions” clearly produce hallucinatory experiences characterized by clarity of thought, euphoria, and the ‘realness’ feel of the experience. As James E. Whinnery has reported, hypoxic G-LOC episodes have some similarities to NDEs, such as floating sensations, OBEs, visions of lights, and “vivid dreamlets of beautiful places that frequently include family members and close friends, pleasurable sensations, euphoria, and some pleasurable memories” (Greyson, “Near-Death” 334). The ability to consistently induce these dreamlets in pilot centrifuges should have dispelled the myth that hypoxic hallucinations are nearly always frightening, confused, or disoriented. And the prevalence of visions of the deceased in NDEs is not surprising: patients who merely have delirium are not dying and have no particular expectation of dying. For the same reason, it should not be surprising that G-LOC dreamlets do not share other NDE features. The context of NDEs is much different, as the sensation or expectation of dying is much more likely in near-death contexts. And while Greyson points out that NDErs who had hallucinations prior to their NDEs describe their NDE worlds as “‘more real’ than the world of waking hallucinations” (334), the proper comparison is between NDEs and (very vivid and realistic) hallucinations that follow a loss of consciousness (e.g., dreams), not waking hallucinations.
In their prospective study of NDEs published in Lancet, Pim van Lommel and colleagues argue that NDE-like hallucinations induced in the laboratory are simply too fragmented to be comparable to NDEs (van Lommel et al. 2044). So why do NDErs recall such vivid experiences, rather than fragments of memories, if NDEs are hallucinations? Fox suggests that the answer does not lie in what is happening to the brain during the NDE, but in how NDE reports are reshaped afterward:
[I]t is clearly probable that both the structured story which at least some NDErs tell and its vividness and clarity may both stem from a variety of sources other than the purely private experiences of the NDErs themselves…. [P]lot and detail may potentially hail from a wide range of sources, including … the behavior of near-death researchers themselves as they attempt to draw out a story along already existing and fixed lines, and the processes which have been seen to exist when the NDEr’s story is told and retold before groups (which may themselves interact in the process of composition and reshaping of the original traveller’s tale) (Fox 203).
In fact, the comments of NDErs themselves provide evidence that NDE accounts become more elaborate over time while NDErs’ commitment to the reality of their experiences deepens. After 23 years of trying to determine the significance of her NDE, one woman commented: “It was real then. It is more real now” (Zaleski, “Otherworldly” 150). Another NDEr noted that what he understood and remembered about his NDE had grown over the years by relating the story to others (150). In one of the more reliable studies of NDE incidence and transformation, van Lommel and colleagues found that the transformations widely believed to occur after NDEs actually do occur[8], but that “this process of change after NDE tends to take several years to consolidate” (van Lommel et al. 2043). In other words, the transformative effect of NDEs on experients is not immediate, but gradual.[9] This suggests that NDE transformations do not result from the NDE itself, but from reflecting on the meaning of the experience—that is, from the added layers of meaning and interpretation experients’ place on their NDEs.
Rense Lange, Bruce Greyson, and James Houran have even found suggestive statistical evidence for embellishment. In the process of establishing that the Greyson NDE Scale can reliably diagnose and measure the depth of NDEs, the researchers made a curious discovery about their sample of NDErs. Plotting data on when an NDE occurred against when it was reported, they found that “when reported at a later age (50 years or older) NDE[s] appear more intense then when reported earlier (49 or younger), and the intensity of the reported NDE[s] increased with their latency (shorter vs. longer than 15 years)” (Lange, Greyson, and Houran 168). In other words, the longer the delay between having the experience and reporting it, the more intense the NDE that was reported. As the authors note, however, these findings conflict with those of a similar study by Carlos Alvarado and Nancy Zingrone, and David Lester found no correlation between NDE depth (as measured by Kenneth Ring’s Weighted Core Experience Index) and length of delay between the NDE and when it was reported (172). Consequently, the discovery of embellishment in the Lange-Greyson-Houran study may have been peculiar to that particular sample of NDErs, rather than a finding that should be generalized to all NDErs. The authors suggest longitudinal studies to definitively determine the extent of embellishment in NDEs (173).[10]
Further evidence that NDE accounts are continually reshaped over time to make them more coherent and interesting comes from comparisons between the NDEs reported by adults and those reported by children. Childhood NDE reports almost always consist only of memory fragments (Morse 68). Both the Fenwicks and Morse found that childhood NDEs tend to be much more fragmentary than those of adults. This makes sense, for children have fewer conceptual resources to draw on and so are much less likely to incorporate unconscious embellishments in their accounts when recalling their NDEs.
Given fragmentary experiences of any sort, the brain will often fill in the gaps with plausible guesses about what happened in the missing intervals in order for an experience to make sense. Human memory relies on plausible after-the-fact reconstructions of events that often incorporate details invented by the subject, details which were never actually experienced. For example, a witness may provide a description of a robber wearing the wrong color of clothing. Since adults have already developed complex ways of making sense of their experiences, while children have comparably simple thought processes, it would not be surprising for adult NDErs to unconsciously embellish reports of their experiences with after-the-fact interpretations of them. This seems to be the most likely explanation for why adult NDE reports are so vivid and structured, flowing seamlessly from one NDE element to another, while childhood NDEs tend to be fragmentary.
Van Lommel and colleagues open their discussion of the results of their landmark longitudinal study with an argument against physiological explanations for NDEs:
Our results show that medical factors cannot account for [the] occurrence of [the] NDE; although all [of our] patients had been clinically dead, most did not have [an] NDE. Furthermore, seriousness of the crisis was not related to occurrence or depth of the experience. If purely physiological factors resulting from cerebral anoxia caused [the] NDE, most of our patients should have had this experience (2043).
One possible answer to this argument is anticipated in Blackmore’s model of the NDE: There are different kinds of anoxia, and rate of onset, amount of time before oxygen restoration, and similar factors have to fall within the right ranges before an NDE can take place.[11] Apparently, for the vast majority of cardiac arrest survivors, this does not happen, and so NDEs are rare among them, no matter how close they come to death as measured by some objective criterion. Another possible answer, perhaps complementary to Blackmore’s, is suggested by Britton and Bootzin’s research: If only a small minority of those who come close to death are physiologically predisposed to have NDEs, the vast majority will experience nothing—and this is exactly what we find.
On the other hand, what of the alternative explanation? If NDEs were really glimpses of an afterlife, why is it that only a fraction of those who come close to death (about 10-20% per van Lommel et al.) report them?[12] Physiology provides a ready answer: Woerlee has calculated that around 20-24% of those undergoing cardiopulmonary resuscitation (CPR) have some degree of consciousness restored during CPR, a fraction of whom could be having NDEs precisely because the conditions are ripe for an altered state of consciousness (Woerlee, “Cardiac” 233, 244). And why aren’t NDEs consistently reported (nearly 100% of the time) after the controlled induction of hypothermic cardiac arrest or “standstill,” where patients are clinically dead for up to an hour?[13] The vast majority of those who come as close to death as possible without actually dying experience nothing at all (van Lommel et al. 2041). If NDEs are to be understood as glimpses of an afterlife, are we to conclude that 80% of individuals cease to exist when they die, while the remaining 20% survive bodily death?
While some NDErs claim to accurately see things they could not possibly see from their bodies, such anecdotes are difficult to corroborate, and it would not be surprising if NDErs consciously or unconsciously exaggerated the accuracy of their descriptions in order to validate their experiences. As we shall see later, many NDErs are already known to exaggerate claims about their psychic abilities after their NDEs; so it would not be surprising for them to exaggerate claims about what they saw during their out-of-body experiences as well.
The near-death literature is filled with anecdotes of NDErs providing accurate details about events they could not have possibly learned about through normal means. But as I hope to make clear, claims of unequivocal paranormal perception during NDEs are greatly exaggerated. Let’s take a closer look at a few well-known cases widely held to provide such evidence.
Maria’s Shoe
In 1984 Kimberly Clark (now Kimberly Clark Sharp) reported a sensational case of apparent veridical paranormal perception during an NDE. Seven years earlier, in April 1977, an out-of-town migrant worker known only as “Maria” was admitted to the coronary care unit of Seattle’s Harborview Medical Center after a heart attack. Three days later, Maria had a second heart attack while still hospitalized and was quickly resuscitated. When Clark came to check on Maria’s condition later that day, Maria reported an OBE where she witnessed her resuscitation from above, noting printouts flowing from the machines monitoring her vital signs. Next she reported becoming distracted by something over the area surrounding the emergency room entrance and ‘willing herself’ outside of the hospital. She accurately described the area surrounding the emergency room entrance, which Clark found curious since a canopy over the entrance would have obstructed Maria’s view if she had simply looked out of her hospital room window. Maria then became distracted by something on a third-floor window ledge on the far side of the hospital, ‘willing herself’ to this location as well. From this apparent vantage point, she noted a left-foot man’s tennis shoe on a third-floor window ledge. She described the shoe as dark blue with a worn-out patch over the little toe and a single shoelace tucked under its heel. To corroborate her story, Maria asked Clark to go look for the shoe (Clark 242-243).
Unable to see anything from outside the hospital at ground level, Clark reports, she proceeded to search room-to-room on the floor above Maria’s room, pressing her face hard against the windows to see their ledges. Eventually she came across the reported shoe in one of the rooms, but insisted that she could not see the worn-out toe facing outward or the tucked-in shoelace from inside the room. Clark then removed the shoe from the ledge (243). Kenneth Ring and Madelaine Lawrence hail the report as one of most convincing cases of veridical paranormal perception during NDEs on record:
[T]he facts of the case seem incontestable. Maria’s inexplicable detection of that inexplicable shoe is a strange and strangely beguiling sighting of the sort that has the power to arrest the skeptic’s argument in mid-sentence, if only by virtue of its indisputable improbability (Ring and Lawrence 223).
This case has taken on the status of something of an urban legend, allegedly demonstrating that Maria learned things during her OBE that she could not have possibly known about other than by actually leaving her body. But as Hayden Ebbern, Sean Mulligan, and Barry Beyerstein make clear, the details Maria reported were in fact quite accessible to her through ordinary sense perception and inference.
In 1994 Ebbern and Mulligan visited Harborview to survey the sites where the NDE took place and to interview Clark. They were unable to locate “Maria” or anyone who knew her personally and suspect that she is now deceased (Ebbern, Mulligan, and Beyerstein 30). They examined each of the details of Clark’s report and found the case much less impressive than it has been made out to be. First, after being hospitalized for three days, Maria would have been quite familiar with the equipment monitoring her; so her perception of the printouts during her OBE may be nothing more than “a visual memory incorporated into the hallucinatory world that is often formed by a sensory-deprived and oxygen-starved brain” (31). Second, her perception of details concerning the area surrounding the emergency room entrance were of details that “common sense would dictate”—such as the fact that the doors opened inward, accommodating paramedics rushing in patients who need immediate attention (31). Moreover, she was brought into the hospital through this very entrance—albeit at night, but the area was well-lit—and could’ve picked up details about it from normal sensory channels then (31-32). The fact that rushing ambulances would traverse a one-way driveway, too, is something anyone could infer from common sense. Finally, Maria’s hospital room was just above the emergency room entrance for a full three days before she had her OBE, and “she could have [easily] gained some sense of the traffic flow from the sounds of the ambulances coming and going” and from nighttime “reflections of vehicle lights” even if she never left her bed (32).
But what of the most persuasive aspect of her report—her description of the celebrated shoe? How difficult would it have been for her to learn these details without having left her body? Ebbern and Mulligan set out to determine exactly that:
As part of our investigation, Ebbern and Mulligan visited Harborview Medical Center to determine for themselves just how difficult it would be to see, from outside the hospital, a shoe on one of its third-floor window ledges. They placed a running shoe of their own at the place Clark described and then went outside to observe what was visible from ground level. They were astonished at the ease with which they could see and identify the shoe.
Clark’s claim that the shoe would have been invisible from ground level outside the hospital is all the more incredible because the investigators’ viewpoint was considerably inferior to what Clark’s would have been seventeen years earlier. That is because, in 1994, there was new construction under way beneath the window in question and this forced Ebbern and Mulligan to view the shoe from a much greater distance than would have been necessary for Clark (32).
As the authors note, what was a construction area for them in 1994 was a high-traffic parking lot and recreation area back in 1977, providing an even better view of Maria’s shoe than the one they saw so easily. Their 1994 ‘test shoe’ was so conspicuous, in fact, that by the time they returned to the hospital one week later, “someone not specifically looking for it” had noticed it and removed it (32). It is quite likely, then, “that anyone who might have noticed the shoe back in 1977 would have commented on it because of the novelty of its location” and Maria could have heard such a conversation and consciously forgotten about it, incorporating it into her out-of-body imagery (32). Moreover, even if no one had seen it from the ground level, Ebbern and Mulligan tested Clark’s claim that Maria’s shoe was impossible to see from inside the room unless she pressed her face hard against the glass looking for it. This claim was found to be wanting:
They easily placed their running shoe on the ledge from inside one of the rooms and it was clearly visible from various points within the room. There was no need whatsoever for anyone to press his or her face against the glass to see the shoe. In fact, one needed only to take a few steps into the room to be able to see it clearly. To make matters worse for Clark’s account, a patient would not even need to strain to see it from his or her bed in the room. So it is apparent that many people inside as well as outside the hospital would have had the opportunity to notice the now-famous shoe, making it even more likely that Maria could have overheard some mention of it (32).
The authors add that anyone who did press his or her face against the glass to get a closer look at the conspicuous shoe from inside the room could easily see the worn-out little toe and tucked shoelace: “we had no difficulty seeing the shoe’s allegedly hidden outer side” (32). They conclude:
[Maria’s shoe] would have been visible, both inside and outside the hospital, to numerous people who could have come into contact with her. It also seems likely that some of them might have mentioned it within earshot….
[And Clark] did not publicly report the details of Maria’s NDE until seven years after it occurred. It is quite possible that during this interval some parts of the story were forgotten and some details may have been interpolated…. [Moreover], we have no way of knowing what leading questions Maria may have been asked, or what Maria might have “recalled” that did not fit and was dropped from the record (32-33).
Furthermore, Clark’s inaccurate account of how difficult the shoe was to see from both inside and out provides evidence that she subconsciously embellished significant details to bolster the apparently veridical nature of the case (33).
Pam Reynolds
As Michael Sabom recounts in Light and Death, in August 1991 a then 35-year-old woman he called “Pam Reynolds” (a pseudonym) underwent an innovative procedure to remove a brain aneurysm. The procedure—inducing hypothermic cardiac arrest or “standstill”—involved lowering Pam’s body temperature to 60°F, stopping her heart and breathing, and draining the blood from her brain to cool it and then reintroduce it. When her body temperature had reached 60°F and she had no electrical activity in her brain, her aneurysm was removed. About 2 hours after awaking from general anesthesia, Pam was moved into the recovery room still intubated (Sabom, “Light” 46-47). At some point after that, the tube was removed from her trachea and she was able to speak. She reported a classic NDE with a vivid OBE, moving through a “tunnel vortex” toward a “pinpoint of light” that continually grew larger, hearing her deceased grandmother’s voice, encountering figures in a bright light, encountering deceased relatives who gave her “something sparkly” to eat, and being ‘returned’ to her body by her deceased uncle (Sabom, “Light” 42-46).
The case was quickly celebrated because of the lack of synaptic activity within the procedure and Pam’s report of an apparently veridical OBE at some point during the operation. But it has been sensationalized at the expense of the facts, facts which have been continually misrepresented by some parapsychologists and near-death researchers.[14] Although hailed by some as “the most compelling case to date of veridical perception during an NDE” (Corcoran, Holden, and James), and “the single best instance we now have in the literature on NDEs to confound the skeptics” (Ring, “Religious Wars” 218), it is in fact best understood in terms of normal perception operating during an entirely nonthreatening physiological state.
Two mischaracterizations of this case are particularly noteworthy, as their errors of fact greatly exaggerate the force of this NDE as evidence for survival after death.[15] First, in their write-up of the first prospective study of NDEs, van Lommel and colleagues write:
Sabom mentions a young American woman who had complications during brain surgery for a cerebral aneurysm. The EEG [electroencephalogram] of her cortex and brainstem had become totally flat. After the operation, which was eventually successful, this patient proved to have had a very deep NDE, including an out-of-body experience, with subsequently verified observations during the period of the flat EEG [emphasis mine] (van Lommel et al. 2044).
Second, in his Immortal Remains—an assessment of the evidence for survival of bodily death—Stephen Braude erroneously describes the case as follows:
Sabom reports the case of a woman who, for about an hour, had all the blood drained from her head and her body temperature lowered to 60 degrees. During that time her heartbeat and breathing stopped, and she had both a flat EEG and absence of auditory evoked potentials from her brainstem…. Apparently during this period she had a detailed veridical near-death OBE [emphasis mine] (Braude 274).
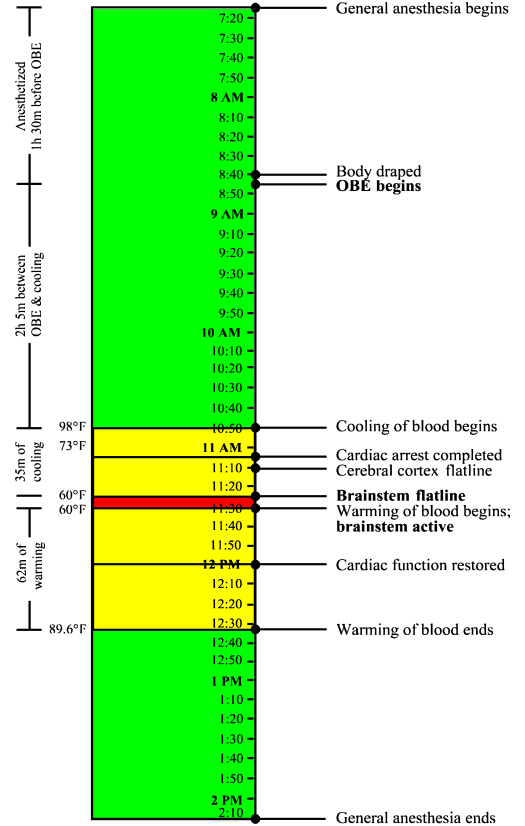
But anyone who gives Sabom’s chapters on the case more than a cursory look will see two glaring errors in the descriptions above. First, it is quite clear that Pam did not have her NDE during any period of flat EEG.[16] Indeed, she was as far as a patient undergoing her operation could possibly be from clinical death when her OBE began.[17] Second, she had no cerebral cortical activity for no longer than roughly half an hour. Both of these facts are nicely illustrated in Figure 1 below.
Despite accurately reporting the facts, Sabom himself has encouraged these misrepresentations.[18] Though he informs the reader that Pam’s experience began well before standstill, he reveals this incidentally, so that a careful reading of the text is required to discern the point. For instance, just after describing Pam’s recollections of an operating room conversation, he notes, almost as an afterthought, that “[h]ypothermic cardiac arrest would definitely be needed” [emphasis mine] (Sabom, “Light” 42). He then goes on to assert that the very features of her experience which cannot be timed happened during standstill. At first, Sabom only implies this by describing the cooling of blood leading to standstill prior to describing the remainder of Pam’s near-death experience (42-46). Then Sabom turns to a discussion of whether Pam was “really” dead during a portion of her standstill state:
But during “standstill,” Pam’s brain was found “dead” by all three clinical tests—her electroencephalogram was silent, her brain-stem response was absent, and no blood flowed through her brain. Interestingly, while in this state, she encountered the “deepest” near-death experience of all Atlanta Study participants….
With this information, can we now scientifically assert that Pam was either dead or alive during her near-death experience? Unfortunately, no. Even if all medical tests certify her death, we would still have to wait to see if life was restored [emphasis mine] (Sabom, “Light” 49).
Of course, the issue of whether Pam was “really” dead within standstill is an extraordinarily misleading red herring in this context. And it is blatantly irresponsible for Sabom to explicitly state that her NDE occurred “while in this state.” As Sabom’s own account reveals, her standstill condition had absolutely nothing to do with the time when we know that her near-death OBE began: A full two hours and five minutes before the medical staff even began to cool her blood, during perfectly normal body temperature![19] (Again, see Figure 1.)
Unlike the other elements of her NDE, we can precisely time when Pam’s OBE began because she did accurately describe an operating room conversation. Namely, she accurately recalled comments made by her cardiothoracic surgeon, Dr. Murray, about her “veins and arteries being very small” (Pam’s words) (Sabom, “Light” 42). Two operative reports allow us to time this observation. First, in the head surgeon’s report, Dr. Robert Spetzler noted that when he was cutting open Pam’s skull, “Dr. Murray performed bilateral femoral cut-downs for cannulation for cardiac bypass” (185). So at about the same time that Dr. Spetzler was opening Pam’s skull, Dr. Murray began accessing Pam’s blood vessels so that they could be hooked up to the bypass machine which would cool her blood and ultimately bring her to standstill. Second, Dr. Murray’s operative report noted that “the right common femoral artery was quite small” and thus could not be hooked up to the bypass machine. Consequently, Murray’s report continues, “bilateral groin cannulation would be necessary: This was discussed with Neurosurgery, as it would affect angio access postoperatively for arteriography” (185). And although Pam’s mother was given a copy of the head surgeon’s operative report (which she said Pam did not read), the report did not say anything about any of Pam’s arteries being too small (Sabom, “Shadow” 7).
Many have argued that Pam’s accurate recall of an operating room conversation is strong evidence that she really did leave her body during the procedure. But there is at least one peculiar fact about Pam’s recollections—in addition to the timing of her experience—which makes a physiological explanation of her OBE much more likely.
General anesthesia is the result of administering a trio of types of drugs: sedatives, to induce sleep or prevent memory formation; muscle relaxants, to ensure full-body paralysis; and painkillers. Inadequate sedation alone results in anesthesia awareness. Additionally, if insufficient concentrations of muscle relaxants are administered, a patient will be able to move; and if an inadequate amount of painkillers are administered, a patient will be able to feel pain (Woerlee, “Anaesthesiologist” 16). During a typical surgical procedure, an anesthesiologist must regularly administer this trio of drugs throughout the operation. But just prior to standstill, anesthetic drugs are no longer administered, as deep hypothermia is sufficient to maintain unconsciousness. The effects of any remaining anesthetics wear off during the warming of blood following standstill (G. Woerlee, personal communication, November 8, 2005).
About one or two in a thousand patients undergoing general anesthesia report some form of anesthesia awareness. That represents between 20,000 and 40,000 patients a year within the United States alone. A full 48% of these patients report auditory recollections postoperatively, while only 28% report feeling pain during the experience (JCAHO 10). Moreover, “higher incidences of awareness have been reported for caesarean section (0.4%), cardiac surgery (1.5%), and surgical treatment for trauma (11-43%)” (Bünning and Blanke 343). Such instances must at least give us pause about attributing Pam’s intraoperative recollections to some form of out-of-body paranormal perception. Moreover, for decades sedative anesthetics such as nitrous oxide have been known to trigger OBEs.
Sometime after 7:15 AM that August morning, general anesthesia was administered to Pam Reynolds. Subsequently, her arms and legs were tied down to the operating table, her eyes were lubricated and taped shut, and she was instrumented in various other ways (Sabom, “Light” 38). A standard EEG was used to record activity in her cerebral cortex, while small earphones continuously played clicks[20] into her ears to invoke auditory evoked potentials (AEPs), a measure of activity in the brain stem (39).
Sabom considers whether conscious or semiconscious auditory perceptions were incorporated into Pam’s OBE imagery during a period of anesthesia awareness, but dismisses the possibility all-too-hastily:
Could Pam have heard the intraoperative conversation and then used this to reconstruct an out-of-body experience? At the beginning of the procedure, molded ear speakers were placed in each ear as a test for auditory and brain-stem reflexes. These speakers occlude the ear canals and altogether eliminate the possibility of physical hearing (Sabom, “Light” 184).
But is this last claim really true? Since Sabom merely asserts this (and has an obvious stake in it being true), we have little reason to take him at his word—especially on such a crucial point. What is the basis for his assertion? Does he have any objective evidence that the earphones used to measure AEPs completely cut off sounds from the external environment?
Since Sabom does not back up this claim in Light and Death, I did a little research and discovered that his claim is indeed false. According to the National Institute of Neurological Disorders and Stroke, as a matter of procedure, a patient who is monitored by the very same equipment to detect acoustic neuromas (benign brain tumors) “sits in a soundproof room and wears headphones” (NINDS). But a soundproof room would be unnecessary, of course, if the earphones used to measure AEPs “occlude the ear canals and altogether eliminate the possibility of physical hearing.” It is theoretically possible that the earphones used in 1991 made physical hearing impossible, whereas the earphones used today do not. However, it highly unlikely, as it would be far cheaper for medical institutions to continue to invest in the imagined sound-eliminating earphones, rather than soundproofing entire rooms to eliminate external sounds. As Gerald Woerlee points out, “earplugs do not totally exclude all external sounds, they only considerably reduce the intensity of external sounds,” as demonstrated by “enormous numbers of people … listening to loud music played through earplugs, while at the same time able to hear and understand all that happens in their surroundings” (Woerlee, “Pam”).
After being prepped for surgery, Pam’s head was secured by a clamp. By 8:40 AM, her entire body was draped except for her head (the site of the main procedure) and her groin (where blood vessels would be hooked up to the bypass machine to cool her blood). In the five minutes or so to follow, Dr. Spetzler would open her scalp with a curved blade, fold back her scalp, then begin cutting into her skull with a Midas Rex bone saw (39-41). At this point, about an hour and a half after being anesthetized, Pam’s OBE began (185). She reported being awakened by the sound of a natural D, then being “pulled” out of the top of her head by the sound (41).
“But,” Sabom asks, “was Pam’s visual recollection from her out-of-body experience accurate?” (186). That is indeed the question to ask regarding the veridicality of her report.
Pam reported that during her OBE, she was able to view the operating room from above the head surgeon’s shoulder, describing her out-of-body vision as “brighter and more focused and clearer than normal vision” (41). In her report of the experience, she offered three verifiable visual observations. First, she said that “the way they had my head shaved was very peculiar. I expected them to take all of the hair, but they did not.” Second, she reported that the bone saw “looked like an electric toothbrush and it had a dent in it, a groove at the top where the saw appeared to go into the handle, but it didn’t.” Finally, she noted that “the saw had interchangeable blades … in what looked like a socket wrench case” (41). Subsequently, she only reported auditory observations—hearing the bone saw “crank up” and “being used on something”—but most notably the operating room conversation initiated by Dr. Murray.
Given such vivid ‘perceptual capabilities’ during her OBE, we would expect there to be no confusion about what Pam saw during the experience. So her visual observations provide an interesting test of the notion that her soul left her body while under general anesthesia during normal body temperature. Let us look at each of these in turn.
First, there is the observation that only part of her head was shaved. Perhaps she could have guessed this at the time of her experience, but there is no need even for this in order to account for the reported observation. Surely Pam would have noticed this soon after awaking from general anesthesia—by seeing her reflection, feeling her hair, or being asked about it by visitors. And she certainly would have known about it, one way or the other, by the time she was released from the hospital. Indeed, if her hair had been shaved presurgery, or at any time prior to her general anesthesia, she would have known about it well before her OBE. And patients undergoing such a risky procedure are standardly given a consent briefing where even the cosmetic effects of surgery are outlined—if not explicitly in a doctor’s explanation, then at least incidentally in any photographs, diagrams, or other sources illustrating what the procedure entails. So Pam may have learned (to her surprise) that her head would be only partially shaved in a consent briefing prior to her experience, but ‘filed away’ and consciously forgot about this information given so many other more pressing concerns on her mind at the time. That would be exactly the sort of mundane, subconscious fact we would expect a person to recall later during an altered state of consciousness.[21] And although we are not given the exact date of the operation, Sabom reports that the procedure took place in August 1991 (38). He later tells us that he interviewed Pam for the first time on November 11, 1994 (186). That leaves over three years between the date of Pam’s NDE and Sabom’s interview—plenty of time for memory distortions to have played a role in her report of the experience. So there is nothing remarkable about this particular observation.
Second, there is her description of the bone saw. But the very observation that provides the greatest potential for supporting the notion that she actually left her body during her OBE actually tends to count against that hypothesis. As Sabom recounts,
Pam’s description of the bone saw having a “groove at the top where the saw appeared to go into the handle” was a bit puzzling…. [T]he end of the bone saw has an overhanging edge that [viewed sideways] looks somewhat like a groove. However, it was not located “where the saw appeared to go into the handle” but at the other end.
Why had this apparent discrepancy arisen in Pam’s description? Of course, the first explanation is that she did not “see” the saw at all, but was describing it from her own best guess of what it would look and sound like (187).
Precisely! Except that, of course, Pam didn’t need to guess what the bone saw sounded like, since she probably heard it as anesthesia failed. An out-of-body discrepancy within Pam’s NDE prima facie implies the operation of normal perception and imagination within an altered state of consciousness. Indeed, this explanation is so straightforward that Sabom considers it before all others. And it is telling that the one visual observation that Pam (almost) could not have known about other than by leaving her body was the very detail that was not accurate.
Let us turn to the report of Pam’s final visual observation during her OBE, her comment that the bone saw used “interchangeable blades” placed inside something “like a socket wrench case.” This detail was also accurate; however, one need not invoke paranormal perceptual capabilities to explain it. As Woerlee notes,
[S]he knew no-one would use a large chain saw or industrial angle cutter to cut the bones of her skull open…. Pneumatic dental drills with the same shapes, and making similar sounds as the pneumatic saw used to cut her skull open, were in common use during the late 1970s and 1980s. Because she was born in 1956, a generation whose members almost invariably have many fillings, Pam Reynolds almost certainly had fillings or other dental work, and would have been very familiar with the dental drills. So the high frequency sound of the idling, air-driven motor of the pneumatic saw, together with the subsequent sensations of her skull being sawn open, would certainly have aroused imagery of apparatus similar to dental-drills in her mind when she finally recounted her remembered sensations. There is another aspect to her remembered sensations—Pam Reynolds may have seen, or heard of, these things before her operation. All these things indicate how she could give a reasonable description of the pneumatic saw after awakening and recovering the ability to speak (Woerlee, “Anaesthesiologist” 18).
And, predictably enough, the dental drills in question also used interchangeable burs stored in their own socket-wrench-like cases.
During anesthesia awareness, and as far from standstill as a person under general anesthesia can be, Pam could have heard her surroundings, but not seen them, since her eyes were taped shut. And the facts of her case strongly suggest that this is exactly what happened. Information that she could have obtained by hearing was highly accurate; at the same time, information that was unavailable to her through normal vision was the very information which was inaccurate. More precisely, her visual descriptions were only partially accurate: accurate on details she could have plausibly guessed or easily learned about subsequent to her experience, and inaccurate on details that it would be difficult to guess correctly.
In other words, OBE imagery derived from hearing and background knowledge, perhaps coupled with the reconstruction of memory, fully accounts for the most interesting details of Pam Reynolds’ NDE report. After awakening from inadequate anesthesia by the sound of the bone saw revving up, her mind generated a plausible image of what the bone saw used during her operation looked like, rendered from her prior knowledge of similar-sounding dental drills. But her best guess about the appearance of the bone saw was inaccurate regarding the features of the bone saw that only true vision could discern: whether there was a true groove in the instrument, and where it was located.
Moreover, the fact that Pam’s NDE began during an entirely nonthreatening physiological condition—under general anesthesia at normal body temperature—implies that there was no particular physiological trigger for the experience (such as anoxia/hypoxia). Rather, it appears that her NDE was entirely expectation-driven. Before going into surgery, Pam was fully aware that she would be taken to the brink of death while in the standstill state. Awakening from general anesthesia by the sound of the bone saw appears to have induced a fear response, which in turn caused Pam to dissociate and have a classic NDE. Indeed, this makes sense of her otherwise odd report of being pulled out of the top of her head by the sound of the saw itself.
At least five separate studies (Gabbard, Twemlow, and Jones; Stevenson, Cook, and McClean-Rice; Gabbard and Twemlow; Serdahely, “Variations”; Floyd) have documented cases where fear alone triggered an NDE. As Ian Stevenson, Emily Williams Cook (now Emily Williams Kelly), and Nicholas McClean-Rice conclude, “an important precipitator of the ‘near-death experience’ is the belief that one is dying—whether or not one is in fact close to death” (Stevenson, Cook, and McClean-Rice 45). They go on to label those (otherwise indistinguishable) NDEs precipitated by fear of death alone “fear-death experiences” (FDEs). Physiologically, such NDEs might be mediated by a fight-or-flight response in the absence of an actual medical crisis. In a case reported by Glen Gabbard and Stuart Twemlow, an NDEr dislodged the pin of a dummy grenade he thought to be a live one, producing a classic NDE similar to the one Pam experienced:
A marine sergeant was instructing a class of young recruits at boot camp. He stood in front of a classroom holding a hand grenade as he explained the mechanism of pulling the pin to detonate the weapon. After commenting on the considerable weight of the grenade, he thought it would be useful for each of the recruits to get a “hands-on” feeling for its actual mass. As the grenade was passed from private to private, one 18-year-old recruit nervously dropped the grenade as it was handed him. Much to his horror, he watched the pin become dislodged as the grenade hit the ground. He knew he only had seconds to act, but he stood frozen, paralyzed with fear. The next thing he knew, he found himself traveling up through the top of his head toward the ceiling as the ground beneath him grew farther and farther away. He effortlessly passed through the ceiling and found himself entering a tunnel with the sound of wind whistling through it. As he approached the end of this lengthy tunnel, he encountered a light that shone with a special brilliance, the likes of which he had never seen before. A figure beckoned to him from the light, and he felt a profound sense of love emanating from the figure. His life flashed before his eyes in what seemed like a split-second. In midst of this transcendent experience, he suddenly realized that grenade had not exploded. He felt immediately “sucked” back into his body (Gabbard and Twemlow 42).
Gabbard and Twemlow conclude that “thinking one is about to die is sufficient to trigger the classical NDE” (42). After comparing experiences that occurred in nonthreatening conditions with those where subjects were actually close to death, they also concluded that no particular elements were “exclusive to near-death situations,” but “several features of the experiences were significantly more likely to occur when the individual felt that death was close at hand” [emphasis mine] (42). That expectation alone can trigger NDEs in certain individuals, then, is well-documented.
If Pam had truly been out of body and perceiving, both her auditory and visual sensations should’ve been accurate; but when it came to details that could not have been guessed or plausibly learned after the fact, only her auditory information was accurate. Moreover, it is significant that as her narrative continues beyond the three visual observations outlined above, the remainder of her reported out-of-body perceptions are exclusively auditory. Finally, it is interesting that Pam reports uncertainly about the identity of the voice she heard when her OBE began: “I believe it was a female voice and that it was Dr. Murray, but I’m not sure” (Sabom, “Light” 42).
These facts strongly imply anesthesia awareness, and tend to count against the idea that Pam’s soul left her body during the operation. If her soul had left her body, the fact that her account contains out-of-body discrepancies doesn’t make much sense. But it makes perfect sense if she experienced anesthesia awareness, particularly when one looks at which sorts of information that she provided were accurate and which were not. Pam Reynolds did not report anything that she could not have learned about through normal perception, and this is exactly what we would expect if normal perception alone was operating during her OBE. It is little wonder that Fox concludes that “the jury is still very much out over this case” (Fox 210).
NDEs in the Blind?
As Susan Blackmore reported in Dying to Live, as of 1993, even Kenneth Ring conceded (in his own words) that there hadn’t been a single “case of a blind NDEr reported in the literature where there was clear-cut or documented evidence of accurate visual perception during an alleged OBE” (Blackmore, “Dying” 133). But Blackmore’s unsuccessful search for such cases prompted Ring and a doctoral student, Sharon Cooper, to endeavor upon a search of their own.
The results of their search are published most prominently in their joint 1999 book Mindsight: Near-Death and Out-of-Body Experiences in the Blind. There they document 31 cases of blind persons who had NDEs or OBEs, 10 of which were not medically close to death at the time of their experiences. These cases were garnered from responses to an advertisement in the International Association for Near-Death Studies (IANDS) Newsletter Vital Signs, as well as from contacts in 11 different organizations for the blind. Of the 31 persons in the sample, 14 were born blind, 11 lost their sight after they were five years old, and 6 were highly visually impaired. 25 of the 31 reported visual sensations during their experiences, as did 9 of the 14 persons blind from birth. The most startling claim made in Mindsight is not simply that some blind NDErs testify to gaining knowledge of facts they could only have learned through a faculty like vision, but that relevant eyewitnesses can corroborate their testimony.
But is there actually strong evidence of veridical paranormal perception in Ring and Cooper’s sample of blind NDErs? One reason Fox questions the significance of this study is that those known to acquire sight for the first time, or reacquire it after a very long time, have difficulty making sense of their visual sensations. He notes the case of a 52-year-man who, after receiving corneal grafts, could not visually identify a lathe that he was otherwise well-acquainted with—by touch—unless he was given the opportunity to touch it. Continually frustrated at his inability to interpret his visual sensations, he eventually took his own life a full two years after the operation (Fox 225-226). By contrast, Ring and Cooper’s blind NDErs are said to have “virtually immediately [gained] the ability to perceive accurately just such things as hospitals and streetlights with virtually no difficulty whatsoever” (226). While Ring and Cooper interpret this as evidence of a previously unknown sort of synesthetic perception ‘transcending’ normal human vision (224), Fox points out that more mundane sources—such as learning from mass media or NDE researchers that OBEs, tunnels, and lights are to be expected during near-death crises—might more satisfactorily explain the blind NDErs’ testimonies (239). Irwin notes similar possibilities:
[These cases] may be inspired by accounts of other people’s NDEs that have been widely disseminated in various forms of the media. That is, might a blind person have heard that people see certain things in a near-death encounter and unconsciously generated a fantasy that conformed to this belief?… [Blind NDErs might also] learn about what to expect in an afterlife from diverse sociocultural sources, and they may rely extensively on these expectations in generating a near-death fantasy…. Thus, the blind may commonly have a belief that they will suffer no visual affliction in an afterlife, and this belief may influence the content of NDEs in the blind (Irwin, “Mindsight” 112).
Fox adds that Ring and Cooper’s two most impressive cases are suspect as evidence for paranormal perception in the blind. In one of these cases, for instance, though an NDEr was said to have superior perceptual capabilities—like “omnidirectional awareness” of the environment—her out-of-body ‘perceptions’ were colorblind. But surely, Fox interjects, “we should expect in such a situation to see in colour. Indeed, we might reasonably expect to appreciate more, deeper and greater colour in such a condition, not less colour or none at all” (Fox 232). In the other case, a 33-year-old man reported an NDE when he was 8-years-old. But, Fox adds, one “might seriously question whether the testimony, twenty-five years after the event, of an episode that occurred to an 8-year-old boy, should qualify as one of their two most impressive cases” (231). Most significantly, though, Fox notes the statistical improbability of NDE researchers finding any genuine cases of NDEs in the blind:
Further, the reader may wonder at the statistical improbability of some of the events that Ring and Cooper present. NDEs seem quite rare, despite the recent publicity that has surrounded them. In this context, for example, it is worth noting that a recent study organized by British theologian Paul Badham and neuroscientist Peter Fenwick, which attempted to gain empirical support for the hypothesis that something leaves the body during an NDE, foundered because of a paucity of cases in the hospital chosen for the study. To find NDEs in the blind, therefore, would seem to be an incredibly difficult task. That Ring and Cooper found twenty-one such cases [31 if you include OBEs not near death] is an extraordinary achievement. That one of their two best cases [the colorblind one] was referred by the same social worker [Kimberly Clark] as was involved in the celebrated ‘tennis shoe’ case, and indeed came from the same hospital, seems most striking—and incredibly statistically improbable (Fox 232).
But Fox’s analysis does not end here. What of the alleged cases of veridical paranormal perceptions in these blind NDErs? While Ring and Cooper recognize the need for corroboration from others of the events NDErs report, and indeed present cases claiming exactly that, Fox notes that “a critical reading of the quality of the data presented reveals the need for caution in accepting them unreservedly” (232). He points out, for instance, that in one case passed on to Ring and Cooper by another NDE researcher, no one appears to have ever followed-up with potential witnesses (232). In another seemingly impressive case, a man who had been blind for 10 years reported an OBE after laying down on a couch where he could see a tie that he was wearing purchased for him by a friend who had never described it to him. The NDEr reported how amazed his friend was when he accurately described the patterns on the tie to her (233). But upon interviewing the friend, Ring and Cooper found that she could not really corroborate his recollection:
Although Ring and Cooper present this as a ‘corroborative’ case of sight during a blind respondent’s out-of-body experience, it is clear that it is not. The witness does not remember clearly the events or the tie. She thus cannot corroborate the detail of the episode in question, but merely presents a testimony to Frank’s apparent truthfulness and simply thinks that he was ‘probably accurate’ in the details given…. Once again, therefore, we must exercise care with the quality of the data presented…. More cautious commentators may be forgiven for suggesting that much stronger data are needed before they agree that existing scientific paradigms need to be hauled down and news ones erected (Fox 234).
Thus Blackmore’s conclusion about paranormal perception during NDEs (including NDEs in the blind) prior to Ring and Cooper’s study is just as poignant today as it was over a decade ago:
I think it would not be surprising if there were many claims of paranormal perception in NDEs even if it never happened. It is my impression that it probably never does happen…. [F]or the moment at least, these claims present no real challenge to a scientific account of the NDE (Blackmore, “Dying” 134-135).
NDE Target Identification Experiments
The cutting edge of near-death research lies in controlled tests of veridical paranormal perception during the out-of-body phase of those NDEs that include OBEs. The detection of remote visual targets during out-of-body NDEs has the potential to provide decisive evidence of consciousness functioning independently of the body, conceivably answering the survival question once and for all. Alternatively, if NDErs are given ample opportunities to identify remote visual targets during their experiences yet fail to do so, veridicality studies offer the prospect of confirming the hallucinatory nature of these experiences. Given the importance of such experiments in either establishing or falsifying veridical paranormal perception during NDEs, it would seem remiss to conclude this section without a survey of the results of NDE veridicality research conducted to date.
Thus far there have been five separate studies in which remote visual targets were placed in presumably NDE-conducive hospital environments. Although earlier experiments with OBEs induced at will have failed to provide compelling evidence of any paranormal processes operating during induced OBEs (see Alvarado 199-200 and especially Blackmore, “Beyond” 189-199 & 213-224 for a survey of the results of these experiments), one might anticipate a greater likelihood of paranormal activity during spontaneous out-of-body NDEs. The first NDE target identification experiment was carried out in the mid-1980s by Janice Minor Holden in the emergency room (ER), each room of the coronary care unit (CCU), and each room of the intensive care unit (ICU) at Lutheran General Hospital in Park Ridge, Illinois (Holden and Joesten 46). As Holden and Leroy Joesten report, visual targets were placed
in the corners of hospital rooms in which near-death episodes were most likely to occur…. in such a way as to be visible only from a vantage point of looking down from the ceiling. No living person was to know the exact content of the stimuli, thus rendering the design double-blind. Once the patient was resuscitated from a near-death episode in one of the “marked” rooms, knowledge of the content of the visual stimulus would be assessed (Holden and Joesten 46).
The authors go on to explain what would constitute a positive result in their study: “If [out-of-body NDErs] accurately identified card content with significantly greater frequency than other NDErs and non NDErs … the hypothesis that [out-of-body NDErs] have veridical perception … would be supported” (Holden and Joesten 48). Unfortunately, however, in the entire year of the study, only 1 cardiac resuscitation occurred in the hospital areas covered by the study, to an Armenian immigrant with poor English who declined to give an interview about his resuscitation. At the same time, at least one NDE occurred in a hospital area not covered by the study (Holden and Joesten 51). With no experiences to test, inevitably no positive results were reported.
A second experiment was conducted by Madelaine Lawrence at Hartford Hospital, Connecticut until early November 1994, when Lawrence was Director of Nursing Education and Research. A scrolling LED display placed in the cardiac electrophysiology lab—though occasionally turned off—was up and running for a total of about 6 months (M. Lawrence, personal communication, August 7, 2006). Lawrence reports:
I placed an electronic sign high on a cabinet in the room [of the electrophysiology lab], not visible to anyone standing on the floor. In order to read the sign a person needed to use a ladder or be out of his body. It contained a nonsense statement like, “The popsicles are in bloom,” and I changed it randomly. It was nonsense so that no one could say he overheard a conversation about the words on the sign. All subjects who became unconscious during the EP [electrophysiology] studies were interviewed and asked to describe their experiences. We were hoping they had had an NDE and had read the sign (Lawrence 158-159).
Unfortunately, although “three patients reported the early stages of an out-of-body experience,” no one had an OBE extensive enough to see the sign (159). So the results of this study, too, can only be considered negative.
A third experiment was set up in “the medical, emergency, and coronary care units of Southampton General Hospital” in the United Kingdom by Sam Parnia from August 1997 to August 1998 (Parnia et al. 150; S. Parnia, personal communication, August 3, 2006). For one year “boards were suspended from the ceiling of the wards…. [with] various figures on the surface facing the ceiling which were not visible from the floor” (Parnia et al. 151). Of the 63 cardiac arrest survivors interviewed during that time, 7 had some recall of the period after they lost consciousness. Of these 7, 4 had NDEs as defined by the Greyson NDE Scale, 2 had NDE-like memories (e.g., feelings of peace or seeing deceased relatives), and 1 had memories unlike NDEs (e.g., seeing “some unknown people jumping off a mountain”). Though two of the four NDErs “lost awareness of their bodies,” none of them had full-blown OBEs (151-153).
Under the supervision of neuropsychiatrist Peter Fenwick and Religious Experience Research Centre (RERC) Director Paul Badham, Penny Sartori conducted a fourth target identification experiment, also in the United Kingdom, at Morriston Hospital, Swansea from January 1998 to January 2003 (Sartori 34). As Sartori explains:
At each patient’s bedside in ITU [the intensive therapy unit], mounted on the wall, is a cardiac monitor. Symbols which were mounted on brightly coloured day glow paper to attract attention were placed on the top of each monitor. These symbols were above head height and concealed behind ridges to prevent them being viewed from a standing position, thus ensuring they could only be viewed from an out-of-body perspective (Sartori 35).
Sartori adds that the symbols were inconspicuously changed every two months and covered by a card removed away from her sight, “ensuring that not even the author knew which symbol was on which monitor” (35). Though all ITU patients were interviewed in the first year of the study, for logistical reasons interviews in the remaining four years were limited to cardiac arrest survivors, those who came so close to death that their survival was unexpected, and spontaneous OBErs and NDErs (36). Consistent with van Lommel and colleagues’ findings, about 18% of the cardiac arrest survivors reported NDEs; about 5% of them reported OBEs (37-38). In the entirety of Sartori’s 5-year study, 15 patients reported NDEs or NDE-like experiences, and 8 OBEs were reported (37-38). Nevertheless, Sartori reports, this study also yielded negative results, as “not all of the patients rose high enough out of their bodies and some reported viewing the situation from a position opposite to where the symbols were situated” (Sartori 38).
The fifth and most recent veridicality study was conducted by Bruce Greyson, Janice Minor Holden, and J. Paul Mounsey at the University of Virginia Health System Electrophysiology Clinic from January 2004 to July 2006 in order to demonstrate that “patients during cardiac arrest have perceptions that they could not have had normally from the position of their bodies,” as this would provide profound “evidence for the independent functioning of the mind while the brain was physiologically impaired” (Greyson, Holden, and Mounsey 93). Following Lawrence’s precedent, the University of Virginia study was premised on cardioversion, the controlled administration of an electric shock to the heart to restore normal heart rhythm. But whereas only about 30% of Lawrence’s electrophysiology patients required cardioversion in order to restore a normal heart rhythm (of which 9% reported NDEs) (Lawrence 158), all 25 of the University of Virginia patients experienced at least two episodes of induced cardiac arrest in order to test implantable cardioverters/defibrillators (ICDs) (Greyson, Holden, and Mounsey 90).
During the two-and-a-half-year period of the study, a ceiling-facing laptop computer visible only from a perspective far above eye level was opened and laid flat on top of a cabinet or video monitor before patients entered the procedure room for ICD implantation and testing. The laptop generated clear and simple but unpredictable cartoon animations (e.g., a jumping frog) of varying colors quasi-randomly selected by the computer based on when it was turned on and unknown to any living person prior to the completion of the study (88-89). Although 5 patients (20% of the sample) acknowledged some recall of events while unconscious—such as a sense of timelessness, feelings of peace, vaguely being somewhere unfamiliar, and possibly sensing the presence of a deceased relative—no NDEs were reported, and thus no out-of-body NDEs were available to test (91-92).
Given that controlled studies of veridical paranormal perception during NDEs have only been attempted intermittently and on a small scale, it is imperative that further target identification experiments are simultaneously carried out at multiple hospitals over a period of several years.[22] For, as Sartori notes,
If hundreds of patients report an OBE there is a greater potential for the symbols being viewed. Equally, if hundreds of patients report an OBE but none correctly identify the symbols then it could lead to the conclusion that the OBE is a mind model (Sartori 39).
In a related but hardly surprising development, similar long-term multicenter research has already established that distant prayer (i.e., prayer unknown to the prayed-for) has absolutely no effect on the health of hospitalized patients (Benson et al. 934). If past experience is any guide at all, NDE veridicality research is no more likely to overthrow our current scientific understanding of humanity’s place in the universe. In the meantime, at any rate, existing veridicality research presents no challenge to the current scientific understanding of near-death experiences as hallucinations.
Psychophysiological Correlates
In order to assess the viability of particular psychophysiological models of OBEs and NDEs, it is essential to survey the data collected on those who have undergone such experiences. As will become evident shortly, taken as a whole such studies strongly imply that whatever these experiences are, they are characterized by features that one would expect of internally generated fantasies, but not of any putative “disembodied existence.”
Few dispute that OBEs and NDEs are altered states of consciousness (ASCs)—temporary departures from the normal (alert) waking state. During ASCs, a variety of mental faculties appear to be altered, including arousal, attention, perceptual functions, imagery skills, memory, cognition, and sense of identity. Other ASCs include REM dreaming, hypnagogic and hypnopompic dreams (when falling asleep or waking up, respectively), lucid dreams (where the dreamer is aware that he is dreaming), hypnosis, meditation, religious and mystical experiences, experiences during prolonged sensory deprivation, states induced by psychoactive drugs, and drug or posttraumatic stress disorder (PTSD) flashbacks. Sometimes ASCs follow a period of unconsciousness, but they are often triggered during normal consciousness.
ASCs are typically understood to involve turning one’s attention inward, into the contents of one’s own mind, rather than revealing anything about the external world. For example, dreams are ASCs that are typically understood to call up internally generated imagery; that is, the world encountered during dreaming is not typically taken to involve any real terrain. Similarly, to say that alien abduction experiences involve ASCs (e.g., sleep paralysis) is to imply that such experiences do not really involve extraterrestrials physically kidnapping unlucky human subjects. Thus, insofar as OBEs and NDEs are such altered states, there is already a reasonable presumption that they do not reflect any objective existence outside of the normal physical body. But let us turn to the specific psychological traits of those who have OBEs and NDEs—traits which strongly imply that some psychophysiological model of OBEs and NDEs must be correct.
For instance, statistically significant correlations between dissociation and absorption and both OBEs and NDEs have been discovered. Dissociation is the shutting out of sensory stimuli, while absorption is focusing on the imagination—but they tend to go hand-in-hand (Greyson, “Near-Death” 323). The classic example of dissociation is “highway hypnosis,” daydreaming or consciously focusing on anything other than driving and yet still arriving at your destination, evidently subconsciously engaging in the required driving skills. Nonpathological dissociation exists on a continuum best measured by absorption, the capacity to become highly engrossed in the imagination, including through books or movies (Blackmore 35; Irwin, “Disembodied” 263).
Across studies, dissociation has been consistently positively correlated with OBEs, and a moderate correlation between absorption and OBEs has been uncovered (Alvarado 192-193). OBErs most frequently dissociate from bodily sensations, and those who experience multiple OBEs are particularly prone to such somatoform dissociation (Irwin, “Disembodied” 271). Irwin found that NDErs were more likely to have suffered childhood trauma than non-NDErs, and consequently theorized that NDErs are predisposed to dissociate during unexpected highly stressful situations in order to “escape” from the pain or anxiety of their environments (Irwin, “Dissociative” 99). Similarly, Kenneth Ring and Christopher Rosing found that NDErs have significantly greater dissociative tendencies than non-NDErs, and suggested that childhood trauma makes victims more prone to dissociation and thus NDEs (Ring and Rosing 211).
In multiple studies, OBErs have been found to have a higher capacity for absorption (Irwin, “Flight” 287; Glicksohn 679; Myers et al. 138) and a greater need for absorbing experiences (Irwin, “Flight” 303; Irwin, “Domain” 6) than non-OBErs. Moreover, Irwin discovered that highly absorbed people can artificially induce OBEs more easily than people who are not particularly absorbed (Irwin, “Disembodied” 263). Similarly, NDErs have not only been found to have a higher capacity for absorption than non-NDErs (Twemlow and Gabbard 230), but to have higher levels of absorption the ‘deeper’ their NDEs (Council, Greyson, and Huff). Interestingly, Stuart Twemlow and Glen Gabbard also found that NDErs were more absorbed than those who had OBEs in non-life-threatening conditions (Twemlow and Gabbard 230). This is not surprising given that NDEs are typically more elaborate than OBEs in other contexts.
Other studies have found that fantasy proneness is higher among OBErs than non-OBErs (Alvarado and Zingrone 14; Hunt et al. 1145; Myers et al. 138; Wilson and Barber 372), and that NDErs were not only more fantasy prone than non-NDErs (Twemlow and Gabbard 230), but more highly fantasy prone the deeper their NDEs (Council, Greyson, and Huff). Fantasy proneness is “characterized by a strong investment in fantasy life, vivid hallucinatory ability, intense sensory experience, and excellent eidetic [vivid visual] memory” (Greyson, “Near-Death” 324).
Finally, compared to non-OBErs, OBErs tend to have more hallucinatory experiences (McCreery and Claridge, “Personality” 140), perceptual distortions (McCreery and Claridge, “Hallucination” 743), distortions of body image (Murray and Fox 70), illusory experiences of changes in body size, and floating sensations (Blackmore, “Postal” 235). Overall, the best predictors of OBEs are dissociation, hypnotic susceptibility, absorption, and fantasy proneness (Alvarado 193-194).
Although Ring and Rosing view dissociative tendencies as a psychological defense mechanism to “tune out” physical threats to one’s well-being while simultaneously opening a door to “alternate realities” (Ring and Rosing 217-218, 231), their hypothetical status as a defense mechanism makes much more sense if OBEs and NDEs do not literally involve any form of disembodiment. For instance, both OBErs and NDErs tend to have high rates of absorption—a trait which Irwin notes “might usefully be thought of as a capacity for imaginative involvement” (Irwin, “Disembodied” 263). But whether it is indicative of a predisposition to have OBEs and NDEs or simply a consequence of having them, such a correlation makes little sense if something actually leaves the body during such experiences. For why would psychological mechanisms—as opposed to physiological crises alone—trigger the release of the soul? Conversely, why would literal separation from the body make individuals more prone to fantasize?
Similarly, why should fear alone trigger NDEs, or the sudden onset of fear during OBEs terminate such experiences (Irwin, “Flight” 81), unless their origins are entirely psychophysiological? As Irwin notes:
The sight of the physical body from the outside may terminate the experience, … because of the emotional response (fear, contempt, revulsion) this sight evokes, but also perhaps because attention is diverted back to the body. Another factor commonly bringing an end to the OBE is the physical body’s being touched by someone (Irwin, “Introduction” 222).
Irwin adds that the fact that the vast majority of OBEs are preceded by physical inactivity implies “that a lack of somatic (kinesthetic and proprioceptive) stimulation is an important condition for the OBE” (227). A psychophysiological process makes sense of why some OBEs originate and end due to emotional reactions or the attention given to bodily processes. But if something literally detaches from the body during OBEs, prima facie psychological factors should neither trigger its release nor hasten its return.
More troubling still for the notion that something leaves the body are various correlations between imagery skills and OBEs.[23] Compared to non-OBErs, for instance, Blackmore found that OBErs “are better at detecting the viewpoint from which a three-dimensional object is seen and are better able to switch viewpoints in their imagination” (Blackmore, “Dying” 180), while Anne Cook and Irwin found that OBErs more accurately anticipated the appearance of physical objects when viewed from different perspectives (Cook and Irwin 30). In addition, Blackmore’s OBErs not only reported “clearer and more detailed” imagined viewpoints than her non-OBErs, but were most significantly better than her non-OBErs at “the ability to imagine the room from a position on the ceiling above their own head” (Blackmore, “Where” 61). Moreover, those who habitually dream in a bird’s-eye view or see themselves during their dreams are more likely to have OBEs (Blackmore, “Where” 61; Irwin, “Perceptual” 214). Furthermore, those who can induce OBEs at will have better dream control skills than spontaneous OBErs—a fact anticipated by psychophysiological models given that OBE adepts would be expected to have “mastered” the required psychological abilities compared to “novice” spontaneous OBErs (Alvarado 202). Similarly, Irwin found that OBErs who report more control over their OBEs tend to have better somatic imagery skills than more “passive” OBErs (Irwin, “Flight” 272-273). Blackmore nicely summarizes most of the findings:
OBErs are better than others at switching from one viewpoint to another (especially to the viewpoint above the head), [are] more proficient at producing clear and detailed images from different viewpoints, and tend to use the observer viewpoint in dream recall…. [T]he easiest switch is to a viewpoint above the head, and … an observer viewpoint is more often used in recalling unpleasant dreams (Blackmore, “Where” 64).
Blackmore interprets the greater prevalence of a bird’s-eye view in OBErs’ unpleasant dreams as “support for the idea that perspective is used as an escape from unpleasant situations” (64) among those better at switching perspective, particularly during “cases of severe pain, shock or fear [where] there is a strong incentive to dissociate oneself from the source of the pain” (57). Additional support comes from Twemlow and Gabbard’s finding that among NDErs, those in severe pain immediately prior to their NDEs felt more detached from their bodies, were more likely to ‘see’ their bodies from afar, and were more likely to ‘occupy’ the environment surrounding their bodies (Twemlow and Gabbard 230).
That various medical factors affect the content of NDEs is equally difficult to reconcile with the notion that NDEs are transcendental journeys. Studies of medical influences on NDE content have found that cardiac arrest NDEs are more likely to feature a sense of power and an awareness of deceased persons, while NDEs resulting from accidents are more likely to feature feelings of joy and little desire to return to the body (Twemlow and Gabbard 230; Twemlow, Gabbard, and Coyne 136). A greater sense of dying among cardiac arrest NDErs might trigger visions of the deceased, while unexpected accidents trigger maximally ‘escapist’ detached indifference.
Plausible psychophysiological reasons for other correlations are not as easy to conjecture, but no less problematic for survivalist interpretations. For example, NDEs during cardiac arrest or while anesthetized are more likely to feature tunnel experiences and experiences of light (Drab 147; Owens, Cook, and Stevenson 1176; Twemlow and Gabbard 230; Twemlow, Gabbard, and Coyne 136), while NDEs resulting from the perception of imminent threats (e.g., in mountain-climbing accidents) in the absence of actual medical crises more often feature feelings of euphoria, thought speeding up, time slowing down, and life review (Noyes and Kletti 57-58; Stevenson and Cook 454). In one study, NDErs under the influence of drugs were also more likely than other NDErs to report an awareness of and communication with other beings, suggesting that drugs directly altered the content of their experiences (Twemlow and Gabbard 230). But if NDEs occur when consciousness is released from the confines of the brain, then altering brain chemistry ought not have an effect on NDE content. Though medical factors affecting a person’s brain state would not be expected to influence the course of a ‘brain-free’ experience, we nevertheless find medical influences on the content of OBEs and NDEs.
Of course, none of these findings are inconsistent with the view that something leaves the body during OBEs and NDEs. But they are clearly not predicted by that view, whereas such correlations are anticipated by psychophysiological models. Those who insist upon a survivalist interpretation of such experiences can surely fit these findings within their particular theoretical frameworks. But prima facie, existing studies of the traits of OBErs and NDErs make psychophysiological models of such experiences much more likely to be true than their transcendental alternatives. That is, extant research strongly implies that OBEs are just one of many different kinds of distortions of body image along a continuum of altered states of consciousness.
What are Out-of-Body Experiences?
But now it is time to return to the question prefacing this section. What, exactly, are OBEs? Several theories have been postulated, but three are particularly promising. The first is Irwin’s theory:
Circumstances associated with extreme (either high or low) levels of cortical arousal evoke a state of strong absorption, particularly in the case of a person with a requisite level of absorption capacity and need for absorbing experiences…. If this state of absorbed mentation is paralleled by a dissociation from somatic (somaesthetic and kinesthetic) stimuli, an OBE may occur (Irwin, “Disembodied” 272).
In other words, OBEs are a form of “dissociation between sensory processing of somatic (somaesthetic and kinesthetic) events and the sense of self or identity” characterized by a high level of absorption (265). Though this theory is based on Irwin’s own findings over the years, Etzel Cardeña’s independent studies confirm that disruptions in sensory input are underlying causes of OBEs, influenced by the hypnotizability and attentional deployment of the subject (Alvarado 204).
A second intriguing theory has been developed by Blackmore: Under stress or when sense input is disrupted, one’s normal model of reality is replaced by one based on memory and imagination. OBEs, perceptual distortions, lucid dreams, and other ASCs are all different models of reality (Alvarado 202). Several confirmed predictions support this theory. First, OBErs should have better imagery skills than non-OBErs, particularly those involving manipulating one’s spatial perspective (202). And as already noted, OBErs are indeed better at identifying the viewpoints of placed objects and imagining changes in perspective. Second, those who induce OBEs at will should have better visual-spatial skills than those who have OBEs spontaneously; and again Blackmore found this to be the case for dream control (202). Third, bird’s-eye-view dreamers should be more likely to have OBEs than those who dream from other perspectives—as both Irwin and Blackmore have found (202-203). Finally, OBErs should have more hallucinations and ASCs than non-OBErs; and four separate studies have confirmed this to be the case (203).
A third interesting theory has a more physiological focus. Few consistent findings on correlations between OBEs or NDEs and physiological factors have been found, but those that have been discovered implicate the temporal lobe in such experiences (see Is the Temporal Lobe Implicated in NDEs? below). Silvia Bünning and Olaf Blanke envision OBEs as “culturally invariant neuropsychological phenomena or deviant self models” resulting from abnormal brain activity centered around the temporo-parietal junction (Bünning and Blanke 332). This unusual neural activity is surmised to produce a dual failure of multisensory integration that leads to an OBE. Conflicting proprioceptive, tactile, and visual information, coupled with a conflict between the vestibular feeling of where the body is and the visual representation of the body’s location, yields an OBE:
[D]uring an OBE the integration of proprioceptive, tactile, and visual information of one’s body fails due to discrepant central representations by the different sensory systems. This may lead to the experience of seeing one’s body … in a position (i.e., on a bed) that does not coincide with the felt position of one’s body (i.e., under the ceiling …) (Bünning and Blanke 334).
Bünning and Blanke argue that just as the phantom limb phenomenon exemplifies a tactile body part illusion, OBEs exemplify a visual whole body illusion (332). Multisensory disintegration is implicated in at least some OBEs by, among other things, experiments with OBEs induced through electrical stimulation of the brain:
Initial stimulations (n = 3; 2.0-3.0 mA) [of the right angular gyrus] induced vestibular responses, in which the patient reported that she was “sinking into the bed” or “falling from a height”. Increasing the current amplitude (3.5 mA) led to an OBE (“I see myself lying in bed, from above, but I only see my legs and lower trunk”). Two further stimulations induced the same sensation, which included an instantaneous feeling of “lightness” and “floating” about two metres above the bed, close to the ceiling (Blanke et al. 269).
So for one of Blanke’s patients, progressively intensifying the electrical stimulation of the same area of the brain started out with simple vestibular sensations and ended with a full-blown OBE. And electrical stimulation of the right temporo-parietal junction has long been known to induce OBEs (Bünning and Blanke 334; Tong 104-105).
The phenomenology of electrically stimulated “OBEs of neurological origin” is clearly distinct from that of spontaneous OBEs. Unlike most spontaneous OBEs, electrical stimulation of the brain tends to produce OBEs in which patients perceive only parts of their bodies from above and perceive clearly illusory distortions and movements of those parts, where patients do not see the environment surrounding their bodies, and in which the experience lacks the realism, continuity, and stability characteristic of spontaneous OBEs (Holden, Long, and MacLurg 102-103; Neppe 89-90). Moreover, spontaneous OBEs seem just as likely to occur in unconscious subjects as conscious ones, but if electrically stimulated OBEs depend upon a conflict between information from the vestibular and visual senses, electrically stimulated OBErs would evidently need to be conscious and perceiving their surroundings with open eyes. And Frank Tong observed that for Blanke’s patient “stimulation applied while the patient’s eyes were closed elicited reports of shifts in perceived body position but failed to elicit out-of-body experiences” (Tong 105).
Vernon M. Neppe noted that he had previously established the existence of four distinct kinds of déjà vu—the common spontaneous form of associative déjà vu, subjective paranormal déjà vu experiences, temporal lobe epilepsy déjà vu, and déjà vu accompanying schizophrenia—and hypothesized that there may be phenomenologically distinct subtypes of OBEs as well (Neppe 92). Perhaps spontaneous OBEs, OBEs induced by relaxation techniques, near-death OBEs, and electrically stimulated OBEs are variants generated by different physiological mechanisms. Alternatively, distinct subtypes might reflect the activation of different parts of a single complex neural mechanism for generating OBEs. On the former hypothesis, multisensory disintegration would be irrelevant to spontaneous, induced, and near-death OBEs, but on the latter, it may well play a role in their production.
One factor implicating multisensory disintegration, particularly vestibular disturbances, is the frequency of spontaneous OBEs in sudden body accelerations or decelerations, such as falls from great heights, car accidents, and sudden altitude changes during flight (Bünning and Blanke 337). The latter is exemplified by the “break-off phenomenon,” where disoriented pilots report a cluster of OBE-like sensations, such as “a feeling of detachment, isolation, and remoteness from their immediate surroundings” (338). Some pilots describe “being all of a sudden outside the aircraft or outside themselves watching themselves while flying the aircraft” (338). And OBEs during flight are most common during absorbing experiences, such as “when pilots are relatively unoccupied with flight details” or on “long cross-country missions over featureless terrain” (338).
Bünning and Blanke classify OBEs as one of three different types of autoscopic phenomena—experiences where one typically sees one’s own body. (Though, as already noted, OBErs do occasionally appear to see from a vantage point near the ceiling without seeing their bodies below.) In autoscopy, a subject feels like he is in his own body and has an internal vantage point, but sees an apparitional mirror image of himself (a double or doppelgänger) in the external environment. In OBEs, a subject feels like he is outside of his body, seeing an image of his normal body and its surroundings from an external vantage point. In heautoscopy, the subject has difficulty localizing where ‘he’ is, sometimes alternating between an ‘internal’ and ‘external’ vantage point, sometimes experiencing both vantage points simultaneously (Bünning and Blanke 333). Whereas in autoscopy the double is typically just an image, in heautoscopy “the double is often experienced as a three-dimensional person” (333). Thus, one feels ‘inside of the body’ in autoscopy, ‘outside of the body’ in OBEs, and simultaneously ‘inside’ and ‘out’—or alternating between them—in heautoscopy (333). The extent to which these experiences are related remains to be seen.
V. Krishnan noted that it is difficult to reconcile the fact that OBErs “nearly always” find themselves looking down on the body from above with the hypothesis that something literally leaves the body during spontaneous OBEs and NDEs:
If the mediator of out-of-body vision is an element that functions independently of the body, I find no reason why it should position itself only above the body; it seems reasonable to expect instances of observation of oneself from other positions to be no less frequent. For example, in the case of a person undergoing an OBE when sitting or standing or falling from a height, self-observation is possible from the front at eye-level or below it (Krishnan 23).
Though subjects are typically sitting or standing during autoscopy and heautoscopy, OBEs predominantly occur when subjects are laying on their backs (e.g., in sleep or general anesthesia). Accordingly, Bünning and Blanke suggest that “OBEs are facilitated by the somato-sensory coding of a supine body position” (Bünning and Blanke 337).
Whichever model turns out to be correct, a preponderance of the evidence suggests that that model will be a psychophysiological one. For if OBEs and NDEs truly represent the detachment of a person’s soul from his body, why would people with certain psychological characteristics have a greater ability to leave the body? If some mechanism can be activated to achieve such a detachment, why would that mechanism have any connection to purely psychological traits? The “projection theory” does not make much sense of the extensive psychological data collected on OBErs and NDErs. But those data clearly makes sense on a psychophysiological understanding of such experiences.
Bodily Sensations
(1) In other NDEs bodily sensations are incorporated into an experience that, on the survivalist interpretation, is assumed to take place in a soul or double that separated from the normal physical body long ago. The Fenwicks report an NDE during a hernia operation where a bodily sensation is felt well into the experience:
I left my body and went walking towards a very bright white light which was at the end of a long tunnel. At the same time I could see three figures standing at the end of the bed and I kept wishing they would go away so that I could go to the light, which to me was lovely and warm. Just as I neared the light I felt a stab in my thigh (Fenwick and Fenwick 91).
With that stab in the thigh this near-death experience ended. But if NDEs were literally journeys of one’s ‘spiritual double’ traveling through the physical world, free of the normal physical body, and entering a tunnel into the afterlife, one should not have any sensations arising from the normal physical body during any part of an NDE.
Also notice that although this NDEr reports leaving his body, ‘walking’ toward a bright light at the end of a long tunnel, and finally getting close to the light, he immediately feels a sharp pain and the experience ends. He does not report ‘backtracking’ through the tunnel and back into his body. At one moment he is close to entering the light, at the next he is back in his bed. If it was necessary for this person’s double to ‘travel’ to get from his body to the light, wouldn’t he have to travel back from the light to return to his body? The lack of a ‘return trip’[24] also suggests that this experiencer was undergoing a hallucination that was suddenly interrupted by a sharp pain.
(2) The Fenwicks provide us with another case where bodily sensations are incorporated into an NDE. While on a Royal Navy ship, a sailor leaning against some chains was accidentally electrocuted when testing the power supply by plugging in a badly connected portable fan. After hearing himself screaming, seeing flashes of electricity ‘licking around’ his body, and hearing a roar, the flashes disappeared and everything went silent. While his body was motionless on the ship’s deck, he reported:
I seemed to be floating in a beautiful velvet-like darkness, feeling completely at peace away from the frightening flashes. I seemed to be going through a tunnel angled slightly downwards when suddenly I found myself standing in a field of beautiful yellow corn…. I felt comfortable and appeared to be wearing a blue gown.
Suddenly, on the distant horizon I saw something that appeared to be a train, in fact a blue train. At first…. I hadn’t noticed gentle music in the background plus the quiet rumble of the blue train.
For some unexplained reason I appeared to get closer to the train, which stopped in front of where I was standing. I could see people in the carriages beckoning to me and telling me to climb aboard….
Then, again almost as if by magic, I was in the train compartment with the faceless passengers, who, I noticed, seemed to be dressed in the same way as I was….
Then it began to happen. I felt a pressure on my shoulders and a strange sensation as I began to rise. It didn’t make any sense—I felt I was being pushed down yet I was going up….
The speed of my ascent became faster and I felt a feeling of anger mixed with regret. I didn’t want to go back. Suddenly I came to and was lying face down on the deck of the frigate passageway. My colleague was pushing on my shoulder blades in the old Holger-Nielson method of resuscitation (Fenwick and Fenwick 154-55).
This NDEr was baffled as to why he felt being pushed down when he was rising up out of a train. But his bodily sensation makes perfect sense if NDEs are brain-generated hallucinations which sometimes incorporate information from the senses, just as a person may dream about going to the bathroom when sleeping with a full bladder.
(3) Remarkably, Morse mentions a childhood NDE that occurred while the child was conscious and talking to nurses—but a person relating an experience to nurses could hardly be supposed to be simultaneously leaving his normal physical body and traveling elsewhere:
Boston Children’s Hospital described a total of 13 pediatric NDEs. Seven of these experiences were told to nurses immediately after recovery, and one was reported during the experience [emphasis mine] (Morse 70).
Unfortunately, Morse provides no further details about this NDE and the researchers who discovered it reported it at a “Perspective on Change” conference at Children’s Hospital in Boston in October 1990. So far as I can determine, there are no published reports about this NDE and Children’s Hospital does not have a written version of this presentation archived.
Living Persons
(1) Some NDErs report seeing living persons in their NDEs while in an ostensibly transcendental realm. The Fenwicks report the case of a woman who encountered her live-in partner after a hysterectomy had caused heavy bleeding and an NDE:
I was outside my body floating overhead. I saw doctors and nurses rushing me along the corridor….
I recall floating in a very bright tunnel. Everything seemed so calm and peaceful. At the end of the tunnel [was] my father, who had died three years previously….
As I said, the feeling of calmness was indescribable. I heard music…. I heard someone calling me. I turned and saw his face at the other end of the tunnel. It was Fabio [the man she was living with]….
Like most people, I had a tremendous fear of death. Now … I have lost that fear of the unknown because I truly believe I have had a preview [brackets original] (Fenwick and Fenwick 32-33).
But Fabio was alive and normally conscious during his girlfriend’s NDE, so he could not have possibly really been calling her inside a tunnel to another world. Clearly we can encounter both the living and the dead in NDEs, just as we can in dreams. This implies that it would be just as irrational to suggest that real people inhabit the NDE world as it would be to suggest that they inhabit the world you encounter in your dreams.
(2) William Serdahely has presented many examples of NDEs that include classic NDE components but which do not quite fit the popularized Moody model of the NDE. For example, Serdahely reports a case of a woman whose NDE was triggered by a sexual assault: “One of the female NDErs saw a living female friend in her ‘windsock’ tunnel. The friend told her to go back to her body” (Serdahely, “Variations” 189). Serdahely provides more details about this NDE as well as a psychological explanation for what triggered it:
The NDE or OBE is tailored specifically to fit the needs of that person. For example, the woman who was sexually assaulted was able to dissociate from the trauma by having an out-of-body experience. The [living] friend she encountered in her experience was a ‘big woman’ who worked for the sheriff’s department that had jurisdiction for the county in which the assault took place and appeared to the NDEr in her sheriff’s uniform (194).
As encounters with living persons repeatedly crop up in NDEs, the less NDEs start to look like visions of another world and the more they appear to be brain-generated hallucinations triggered by a real or perceived threat to the experiencer’s well-being.
(3) Encountering living persons during NDEs is more common in children than in adults. Melvin Morse reports the following NDE of a young Japanese boy:
Japanese children similarly describe simple experiences of seeing a bright light or seeing living teachers and playmates. A 4-year-old boy, who had fulminant pneumonia, described floating out of his body and coming to the edge of a river. His [living] playmates were on the other side, urging him to go back. There was a misty bright light on the other side (Morse 70).
(4) The Fenwicks cite an intriguing case of a childhood NDE which lacked the most common element of the classic NDE—feelings of peace or euphoria—where a living person was also present in the experience. When Richard Hands was 9 years old his appendix was removed but complications led to an NDE:
The first [image I recall] is of looking down on a body on the operating table, being fussed over by green-clad surgeons and nurses. I couldn’t actually see the face—someone was in the way—but I assume it was mine. This image is particularly vivid, and despite its goriness is not associated with any pain or distress, even in recall.
[Then I saw] a blackness with a pinpoint of light far off in the distance. I feel drawn towards the light, but there is a terror and a feeling that I do not wish it to pull me towards it. My [living] mother is with me in this scene, trying to pull me back from the light. There is also a wind rushing past, towards the light (Fenwick and Fenwick 173).
Clearly his mother was not actually present in this ‘blackness’ with light, since she was alive and normally conscious at the time of his experience. Interestingly, this experiencer attached no spiritual significance to his NDE either at the time it occurred or since. Initially he thought it might have been a reaction to the anesthetics he was on at the time, before he had heard of the NDE; now he is inclined to see it as a physiological event that did not depend on anesthetics. He is now a scientific journalist and atheist who is generally skeptical of paranormal claims (173).
In the Fenwicks’ sample only 50% of those who had NDEs when they were between 3-9 years old reported becoming more religious after the experience; by 16 or older this rose significantly to 90% (185). Given that adults have more complex religious concepts than children, it is not surprising that adults are more likely to attach religious significance to an unusual experience that occurred when they narrowly escaped death.
(5) Susan Blackmore reports that a woman who was suffocating after an operation had an NDE where she encountered the medical staff who had been trying to resuscitate her in the light at the end of the tunnel:
[I was] struggling along a dark tunnel in which someone was trying to hold me back. The figures in the bright light at the end of the tunnel proved to be the ward sister and her staff trying to resuscitate me (Blackmore, “Dying” 227).
As Blackmore points out, cases like these don’t “make much sense if you think the beings seen in NDEs are ‘real entities’ inhabiting another realm” (227). But they make perfect sense if NDEs are brain-generated hallucinations. The fact that living persons are occasionally encountered in NDEs severely undermines survivalist interpretations of the NDE.
(6) Interestingly, Serdahely has also found cases where rather prosaic medical imagery was seen in NDEs, though no living persons are reported in this particular account:
One male respondent said he traveled through a tunnel on a cart or gurney on his way to being greeted by his deceased father, godfather, and coworkers, all of whom beckoned him into the light. I had previously come across an NDEr who indicated he had been transported to the light in an ambulance-like vehicle (Serdahely, “Variations” 189).
The Fenwicks report that 14% of their total 350 person sample of NDErs—about 50 people—encountered living persons in their NDEs (the Fenwicks state that 38% of this total sample encountered other persons; a further 38% of those encounters were with living people; hence roughly 14% of the people in his total sample encountered living persons during their NDEs) (Fenwick and Fenwick 79).
Morse and others have found that encounters with living persons are more commonly reported in childhood NDEs than in the NDEs of adults. This is not surprising given that children generally know far fewer people who have died than adults do. While NDEs where living persons are encountered are relatively rare, apparently they still make up a significant fraction of all reported NDEs. As previously noted, the Fenwicks found that more than 1 out of every 10 of their NDErs encountered living persons in their NDEs.
Cultural Differences
(1) In the industrialized West, where Christian imagery dominates, people who encounter religious figures in their NDEs typically encounter Christian religious figures who appear as they are standardly depicted. In one of the Fenwicks’ cases, a woman who reported seeing a light form above her bedroom door just before ‘floating’ over her body encountered Jesus:
Jesus came walking up to me with arms outstretched. He was dressed in a long white robe, his hair to his shoulders, ginger-auburn, and he had a short beard…. I was trying to speak with him but I could only croak because my mouth was dry and my tongue swollen (Fenwick and Fenwick 62).
While we have no idea what the historical Jesus actually looked like, it would be very surprising if he looked exactly as he appears in standard artists’ depictions of him today. The culturally determined appearance of Jesus in this NDE recalls cases of stigmata where the nail wounds of Jesus appear in the hands—exactly where artists’ depictions of Jesus on the cross put them—but not where nails must be placed (in the wrists) in order to successfully crucify someone.
It also seems unlikely that one’s double would suffer astral dry mouth while functioning separately from the normal physical body. But it would not be very surprising to hallucinate having dry mouth while in an imaginary realm.
(2) By contrast, the dominant religious imagery of India is Hindu, and predictably NDEs from India typically involve encounters with recognizably Hindu religious figures. Satwant Pasricha and Ian Stevenson provide us with the following case from one of the largest surveys of non-Western NDEs conducted so far:
Four black messengers came and held me…. [T]he clerks had a heap of books in front of them…. Yamraj was there sitting on a high chair with a white beard and wearing yellow clothes. He asked me, “What do you want?” I told him that I wanted to stay there. He asked me to extend my hand. I don’t remember whether he gave me something or not. Then I was pushed down [and revived] (Pasricha and Stevenson 167).
Here an NDEr is seated near Yamaraj, the Hindu god of death, whose appearance also corresponds to the god’s portrayal in Hindu tradition. While Western NDErs tend to encounter dead friends and relatives more often than religious figures, Hindu religious figures are prominent in NDEs from India. Additionally, we see that NDErs from different cultures also give different reasons for why they are sent back. Western NDErs are often ‘sent back’ in order to take care of immediate family or for some assumed purpose unknown to them; NDErs from India report meeting clerks in an impersonal afterlife bureaucracy who process the dead and send them back because they have been sent the wrong person due to paperwork mistakes (Pasricha and Stevenson 168-169).
(3) Cultural conditioning is even evident in children’s NDEs. In the West, children’s culturally determined encounters with other beings during NDEs tend to be more imaginative than those of adults. Morse paraphrases one girl’s encounter with Jesus during an NDE as follows:
He was in a very bright light that she could not describe other than by saying that it made her feel good. He was sitting there with a round belly and a red hat, looking like Santa Claus (Morse and Perry, “Transformed” 125).
Morse notes that in other cases children have reported encountering wizards, doctors, guardian angels, living teachers, living playmates, pets, and other animals during their NDEs (Morse 70).
(4) Todd Murphy translated 11 published accounts of NDEs in Thailand into English, three of which reported two NDEs from the same subject, yielding a total of 14 cases (Murphy, “Eleven”). Because one of the published accounts was so similar to another, Murphy presented an analysis of 10 of them in his 2001 paper (T. Murphy, personal communication, January 24, 2006). Like NDEs from India, Thai NDEs contrast starkly with those reported in the West.
For instance, like Indian NDErs, Thai NDErs are far more likely to encounter religious figures than deceased friends and relatives: in 9 out of 10 accounts Thai NDErs met Yamatoots, messengers of the god of death Yama (Murphy, “Thailand” 164). And in half of the accounts Thai NDErs reported “being told that they were the wrong person, and being ordered back to life” (175). While deceased friends and relatives are sometimes encountered in Thai NDEs (in 4 of the 10 accounts), rather than greeting the NDEr (as in the West), they inform the NDEr “of the rules governing the afterlife” (175).
While OBEs are rather common early on in Western NDEs, being visited by a Yamatoot is “the most common initial phase” of Thai NDEs (170). Where OBEs do occur, “OBEs in Thai NDEs tend immediately to precede meetings with Yamatoots” (171). Tunnels are “largely absent in Thai NDEs” (with one exception unlike Western tunnel experiences), and feelings of peace or euphoria and experiences of light have not been reported at all (172). Thai NDErs are sometimes judged, but their deeds are recounted by reviewing written records of their lives or the testimony of others. The following case is typical:
I … found myself in the judgment hall of Yama’s palace. I knew that they were ready to judge me for my sins. A giant rooster appeared who told Yama that I had killed him. He emphasized that I had tried to kill him again and again. The rooster also said that he remembered me exactly. An entire flock of roosters also [appeared] and testified that I had killed them, as well. I remembered my actions, and I had to admit that the roosters had told the truth. Yama said that I had committed many sins, and sentenced me to many rebirths both as a chicken, and many other types of birds as well…. But, quite suddenly, an enormous turtle appeared. It screamed at Yama, saying “Don’t take him; he is a good human, and should be allowed to live.” Yama answered the turtle “What did he do to help you?” [ellipses original] (Murphy, “Thailand” 167).
Unlike Western cases, life events are not viewed or relived as flashbacks. Landscapes are common in Thai NDEs, but typically unpleasant, as in the tours of the various hells. And while “Western NDErs may reach a ‘point of no return’ and choose to return to life, Thai NDErs are typically told they were taken because of a clerical mistake and told to return to the body” (177).
Given such stark phenomenological differences, Murphy concludes:
The fact that Thai (and Indian) NDEs do not follow the typical Western progression reflected by Kenneth Ring’s temporal model seems to rule out the possibility that there is an ideal or normal NDE scenario, except within a particular cultural context (169).
Bolstering this point, Murphy adds that “Accounts of Western NDEs would seem to be useless in helping Thais know what to expect at their deaths” (170). He nevertheless concedes vague cross-cultural commonalities “in which individuals commonly use culturally-derived patterns to confabulate individualized death-process phenomena that serve common psychological functions” (177). Such commonalities may reflect common beliefs across societies, such as the idea of postmortem judgment for earthly behavior, tied to an expectation or sense of being dead accompanying NDEs.
(5) Journalists Hiroshi Tanami and Takashi Tachibana originally presented an investigation of 46 Japanese NDEs on NHK television (Morse 70; Tachibana Vol. 2 90). Tachibana subsequently expanded the investigation to that of 243 NDEs (some individuals reported multiple NDEs) discussed in the Japanese-language book Rinshi Taiken (Near Death Experience)[25], which includes a section on the cultural differences between Japanese and other NDEs (Tachibana vol. 2 80-91). The study confirmed that Japanese NDErs often report “seeing long, dark rivers and beautiful flowers, two common symbols that frequently appear as images in Japanese art” (Mauro 57).
In a tabulated chart, 73 reports noted an affective component which was predominantly positive: 32 included being at peace and another 32 included feeling happy, while only 9 were fearful. Leaving the body was reported in 59 NDEs. Of forty-five experiences of light, 16 were preceded by travel through a tunnel. Altogether 30 tunnel experiences were reported, implying that some experiences of light preceded (as in the Tatsuo Katayama case) or did not accompany tunnel experiences. 24 NDEs included encountering darkness. In 153 accounts there was an encounter with others, most commonly with friends or relatives, but also occasionally with otherworldy beings or religious figures. 6 NDEs included reviews of the events of the NDErs’ lives. Landscape visions were most consistent between accounts, with reports of a field of flowers in 102 NDEs. Of the eighty-two NDEs featuring a border, 70 NDEs featured rivers, 6 featured a sea or lake, and 6 featured a gate or wall. In 72 accounts a reason for the NDErs’ return was given: In 37 cases NDErs were “brought” back to life, in 23 they were told to return, and in 12 they chose to return (Tachibana vol. 2 89).
Tachibana had noted that, unlike Western NDEs, the “light is not a personal (or personified) existence…. [It] is an indescribably beautiful and natural light, yet is just light” (Tachibana vol. 2 81, trans. O. Carter), and that there was not a single instance of a Japanese NDEr having any sort of communication with the light. Nevertheless, occasional similarities between these Japanese NDEs and typical Western cases are fascinating exceptions to the general rule of cultural diversity. By the time of their collection in the 1990s, it is hard to say whether the popularization of common Western NDE features had influenced Japanese reports in this ‘East meets West’ society. It is nevertheless notable that one Japanese NDEr recounted an experience dating back to World War II in which he began reviewing his childhood memories before he lost consciousness and had an NDE (Tachibana vol. 1 452-453).
In contrast to the Tachibana study, Yoshia Hata and collaborators at Kyorin University interviewed 17 patients who went into comas with “minimal signs of life” after heart attacks, strokes, asthma attacks, and drug poisoning. 8 of the 17 reported ‘dreams’ where rivers and ponds were prominent, while the remaining 9 had no experiences. 5 of the 8 NDErs reported “fear, pain and suffering,” unlike typical NDEs from the West. While one of the patients from the Kyorin study reported repeatedly doing handstands in the shallows of a reservoir,
Another patient, a 73-year-old woman with cardiac arrest, saw a cloud filled with dead people. ‘It was a dark, gloomy day. I was chanting sutras. I believed they could be saved if they chanted sutras, so that is what I was telling them to do.’ (Hadfield 11).
(6) University of Zambia physician Nsama Mumbwe collected 15 NDE reports from Africa in order to determine if the elements of the prototypical Western NDE were cultural products of the Western media (Morse and Perry, “Transformed” 120-24).
In one case, after being attacked by a lioness protecting her cubs, a 60 year old truck driver reported that a highway opened up for him going endlessly into the sky, surrounded by stars; when he tried to go on to the highway, the stars blocked his way, and he stood there until the highway and stars disappeared (Morse and Perry, “Transformed” 122).
In another African case, an 85 year old woman reports an NDE that sounds a little more like a prototypical Western NDE:
I was suffering from a stroke. During this time I felt I was put into a big calabash [the hollow shell of a gourd] with a big opening. But somehow I couldn’t get out of it. Then a voice from somewhere said to me, ‘be brave. Take my hand and come out. It is not yet your time to go.’
After some time of being in the calabash I managed to get out on my own [brackets original] (Morse and Perry, “Transformed” 122-123).
In the first case the man attributed his NDE to a ‘bad omen’; in the second the NDEr thought someone was trying to ‘bewitch her’ into death. Clearly these are culture-bound interpretations of the experience; but what of the reports of what was experienced?
The single report of being caught inside of a calabash or ‘hollow gourd’ with a large opening has widely been interpreted as a tunnel experience, but it may indicate feeling caught inside of something more like a bottle with only one opening, rather than something more tunnel-like with two openings. After all, the report explicitly refers to a single large opening rather than two openings. So we have a single African NDE which may or may not include a tunnel experience. There is little reason to describe the other African case where a ‘highway’ through the stars opens up as either a tunnel experience or an OBE, since there is no indication of enclosure or of looking down on one’s body or the ground.
(7) In the South Pacific region known as Melanesia, the province of Western New Britain lies just east of mainland Papua New Guinea. Here even the hunter-gatherer culture of the Kaliai cannot escape the influence of Western globalization. In her survey of near-death experiences from this region, anthropologist Dorothy Counts found that the NDE world “is a land that is described as having factories and wage employment. It has an appearance that reminds me of the view approaching Los Angeles from the air” (Counts 130).
One Kaliai NDEr reported walking through a flower field to a road that forked in two. In each fork of the road a man was standing persuading the NDEr to come with him (119-120). The NDEr picked one of the forks at random and he and his guide traveled to a village:
The man took my hand and we entered a village. There we found a long ladder that led up into a house. We climbed the ladder but when we got to the top I heard a voice saying, “It isn’t time for you to come. Stay there. I’ll send a group of people to take you back.”….
As I was walking around, trying to see everything, they took hold of me and took me back down the steps. I wanted to go back to the house, but I couldn’t because it turned and I realized that it was not on posts. It was just hanging there in the air, turning around as if it were on an axle. If I wanted to go to the door, the house would turn and there would be another part of the house where I was standing.
There were all kinds of things inside this house, and I wanted to see them all. There were some men working with steel, and some men building ships, and another group of men building cars. I was standing staring when this man said, “It’s not time for you to be here. Your time is yet to come. I’ll send some people to take you back…. [Y]ou must go back.”
I was to come back, but there was no road for me to follow, so the voice said, “Let him go down.” Then there was a beam of light and I walked along it. I walked down the steps, and when I turned to look there was nothing but forest….
So I walked along the beam of light, through the forest and along a narrow path. I came back to my house and re-entered my body and was alive again (120).
The world that the Kaliai encounter in their NDEs conforms to a Kaliai complex of beliefs known as the cargo belief, whose central assumption is that white people are ‘spirit people’ or ancestors that have returned from the dead. This belief complex is partially based on the Kaliai’s awareness of more advanced Western technology, for the Kaliai believe that spirits or ancestors give technology to human beings. In their belief system, the afterlife is “rich with divinely given technology,” including “factories, automobiles, highways, airplanes, European houses and buildings in great numbers, and manufactured goods” (130).
After discovering such major differences in the descriptions of the NDE world encountered in Western and non-Western cultures, Counts concludes:
[T]he place that [people] perceive as being the world of the dead often is a pleasant, happy place. However, the content of paradise varies and seems to be culturally defined…. North Americans and Europeans see a beautiful garden, while Kaliai find an industrialized world of factories, highways, and urban sprawl….
The culturally structured nature of these experiences is consistent with the explanation that out-of-body and near-death experiences are the result of a psychological state known as hypnagogic sleep. The Kaliai data presented here suggest that this, rather than an objectively experienced “life after death,” is the most reasonable explanation for the phenomena (132-133).
How Consistent are NDE Features across Cultures?
Despite a few core elements—such as having an OBE, going through a tunnel, encountering a light, and meeting deceased relatives—descriptions of the world encountered during Western NDEs are nearly as variable as dreams. Even the identity of ‘the light’ is variable: in some cases it has a personality, in others it does not; sometimes it has a specific identity that varies between people—a ‘bright angel’ in one case, Jesus in another; in other cases it is a path or simply the illumination of another world at the other end of a tunnel (Fox 106, 118). Even the function of light in the NDE varies significantly between individuals:
Indeed, as regards the light’s identity, we cannot even … attempt to identify it by function, for it appears to do a number of things … sometimes merely acting as a destination, sometimes lighting the way, sometimes judging, sometimes asking questions, and sometimes simply returning NDErs to where they came from (Fox 140).
So what features, exactly, are thought to be the consistent or core elements of the prototypical Western NDE? The answer you receive depends on which researcher you ask (see Fox 101), but the list below seems to encompass most of the elements suggested by different near-death researchers:
- Feelings of peace or euphoria, lack of pain
- An out-of-body experience (OBE)
- Traveling through a tunnel or darkness from the physical world to an ostensibly transcendental realm
- Encountering a sun-like light
- Meeting others
- A life review where one’s own life events are viewed or relived and sometimes judged
- Seeing some sort of landscape
- Encountering a barrier or threshold between life and death
Because most Western NDEs do not include all of these elements, I will define the prototypical Western NDE as an experience succeeding a real or perceived imminent physical threat containing at least two of the elements listed above. Since prototypical Western NDEs can occur when subjects only think that they are going to die, such NDEs must be defined in terms of their experiential elements rather than their actual proximity to death. Nevertheless, in the bulk of Western NDE accounts the expectation of dying, at least, clearly precipitated the experience. Thus in non-Western contexts an NDE should generally be understood as altered state of consciousness precipitated by either an expectation of dying or actual proximity to death.
Consistency between different Western NDE accounts has been well-established by near-death research. But to determine whether their commonalities can be found in non-Western NDEs, we must search existing non-Western NDE accounts for elements of the prototypical Western NDE. The chart below summarizes whether or not prototypical Western NDE elements were reported in 11 studies of non-Western NDEs:
NDE Elements across Cultures
| Culture; Study; # of NDEs |
Peace | OBE | Tunnel/ Darkness | Light | Meeting others | Life review |
Landscape | Barrier/ Threshold |
| India; Pasricha 1993, Pasricha and Stevenson 1986; total 45 cases |
No | Yes: in only 1 case |
No | No | Yes | No: written records read |
No: office |
No |
| India; Singh, Bagadia, Pradhan, & Acharya 1988; total 10 cases |
No | No | Maybe | Maybe | Yes | No | No | No |
| Thailand; Murphy 1999; 14 cases* |
No | Yes | Yes: in only 1 case |
No | Yes | No: records read, others testify | Yes: gardens, palace, torture chambers | No: Yamatoots force one back |
| China; Zhi-ying and Jian-xun 1992; 32 cases |
Yes | Yes | Yes | No | Yes | Yes | Yes | No |
| Japan; Hata (in Hadfield 1991); 8 cases |
No | No | No | No | Yes | No | Yes: ponds, rivers |
No |
| Japan; Tachibana 2000; 243 cases |
Yes | Yes | Yes | Yes | Yes | Yes | Yes: rivers |
Yes: river |
| Zambia; Mumbwe (in Morse 1992); 15 cases** |
No | No | Maybe: calabash | No | Yes | No | Yes | Yes: stars blocking road |
| Congo***; McClenon 2006; 4 cases |
No | No | No | Yes: in 1 case | Yes | No | Yes: roadside scenery | Yes: a river |
| Melanesia; Counts 1983; 3 cases |
No | No | No: roads |
No: man lit with flashlight |
Yes | No: sorcerers judged |
Yes: urban sprawl |
Yes: door approach thwarted |
| Guam; Green 1984; 4 cases |
No | Yes: OB visits |
No | No | Yes | No | Yes | Yes: door, field entrance |
* Murphy 1999 reviews the accounts of 11 subjects, three of which recount two NDEs.
** Responses based on the 5 African cases reproduced in Morse 1992 (of the 15 collected).
*** McClenon 2006 reviews 8 reports, but only 4 are first-person NDE accounts; the rest are second-hand or are not of NDEs.
For the sake of fidelity, ambiguous NDE cases, unsoundly procured accounts, and case studies of just one account have been excluded from this cross-cultural survey. For instance, whether various historical narratives are accounts of experiences by individuals who were dying or expected to die is unclear, or otherwise their status as unedited, first-person accounts rather than legendary inventions or accretions is dubious. Studies in which contemporary non-Western accounts were derived solely from second-hand sources rather than from interviews with NDErs themselves have also been excluded. Finally, I have excluded data which are likely to have been contaminated by knowledge of Western NDE motifs, such as findings based on responses to advertisements in nonnative languages (e.g., Blackmore, “India”) or on composite accounts of Western NDEs presented to respondents beforehand (e.g., Kellehear, Heaven, and Gao). It is nevertheless worth noting that none of the excluded non-Western historical narratives (Bailey; Becker, “Centrality”; Becker, “Revisited”; Schorer; Wade), second-hand accounts of non-Western NDEs (Osis and Haraldsson), or single non-Western accounts (Berndt and Berndt; Gómez-Jeria; Kellehear, “Hawaiian”; King) report initial euphoria, transitional passage through a tunnel or darkness, encountering a sun-like light, or anything like the Western life review.
In 11 studies of 7 non-Western cultures (with 3 studies in India, 2 in Japan, and 2 in central Africa), very few elements of the prototypical Western NDE are universally present[26]:
- (1) Feelings of peace have only been reported in NDEs from China and Japan, and unfortunately in their published report Feng Zhi-ying and Liu Jian-xun simply tabulated reported elements without including NDErs’ narratives, making it impossible for us to determine how similar the Chinese elements were to prototypical Western ones. A single Thai NDEr did report feeling “a deep sense of beauty” after an OBE, followed by walking down a road, encountering Yamatoots, and desperately trying to escape from them (Murphy, “Eleven”).
- (2) OBEs are widely present, but absent from NDEs in Zambia, the Congo, and Melanesia, and only 1 OBE is reported in the 55 reports of NDEs from India. Moreover, the OBEs from Guam did not involve looking down on one’s body or the area around it, but of out-of-body ‘flights’ to relatives living in America. That OBEs are not universal in NDEs is somewhat surprising, given the ease of imagining a scene from above (Zaleski, “Life” 62-63); but perhaps this is because “not all cultures recognize OBEs as a herald of death” (Murphy, “Thailand” 171).
- (3) Tunnel experiences were virtually limited to NDEs from China and Japan. One NDEr from Zambia may have reported one, depending on whether ‘calabash’ should be interpreted as ‘tunnel,’ and in a tabulated chart three NDErs from India were paraphrased as reporting a “Feeling of intense darkness” which may or may not represent transitional passage (Singh et al. 303). In one Thai account an NDEr encountered a tunnel twice, first as a means to travel to Yama’s hall of judgment, skipped due to ‘bad weather’ (an elevator was taken instead), and then later to “access” the first level of Hell, where people with the “heads of chickens, buffalos, and cows” are encountered (Murphy, “Eleven”); but Thai NDErs typically traverse roads in their NDEs (Murphy, “Thailand” 172).
- (4) An experience of a sun-like light can be found among Japanese NDE reports, but otherwise only a Congo NDEr “saw a bright, dazzling light” (McClenon, “Kongo” 25) and an NDEr from India was paraphrased as reporting “Feeling of bright light and exploding firecrackers” (Singh et al. 303). A “light that was too bright to bear” was seen where “the cries of those being tortured” could be heard in the fourth level of Hell (reserved for arsonists) in a single Thai NDE (Murphy, “Eleven”).
- (5) Meeting others is the only truly universal element found in every non-Western NDE study, but this general element hardly lends support for the existence of any substantial core NDE across cultures, as it would not be surprising to find encounters with others in many hallucinatory human experiences. Moreover, it covers much variation, such as meeting deceased friends or relatives, strangers, religious figures, animals, living persons, and mythological creatures.
- (6) Viewing or reliving one’s own life events was only reported in NDEs from China and Japan, although NDEs from India and Thailand often included readings of written records of the events of one’s life, reflecting traditional Hindu and Thai beliefs (Murphy, “Thailand” 166; Pasricha and Stevenson 168). Thai NDErs were often judged for specific actions and whether their good deeds outweighed their bad ones, but those affected by their actions (including a rooster and a turtle in one case) would testify for or against them. Outside of the limited Chinese and Japanese data, no “memory flashback” life reviews were reported by any non-Western NDEr.[27] One Melanesian NDEr reported witnessing a sorcerer being judged via loudspeaker and destroyed by fire during his NDE, but the NDEr himself never reviewed the events of his own life (Counts 121-122).
- (7) Encountering a landscape of some sort is nearly universal, but absent from NDEs in India, where NDErs typically enter an administrative office and are sent back because the clerks have been sent the wrong person. This motif is also found in Thai NDEs, occasionally preceding landscape visions. The most common features of the Thai NDE world are visions of Yama’s palace, various tortures being inflicted on wrongdoers, and gardens or land strewn with jewels. But NDE landscapes vary considerably across cultures—bodies of water are prominent in NDEs from Japan, fields in NDEs from Guam, and brightly lit cities with factories, cars, roads, planes, and buildings in NDEs from Melanesia.
- (8) A barrier or threshold was reported in NDEs from Japan (a river, sea, gate, or wall), Zambia (stars blocking a highway), the Congo (a river), Melanesia (a house would turn if a door was approached), and Guam (a field entrance, a door, a hill in the distance to which the NDEr was prevented from traveling). In Thai NDEs, Yamatoots often forced NDErs back into their bodies after they were recognized to be the wrong person, but no barrier prevented them from going further, and no choice to stay or return was ever offered.
Of the 8 prototypical Western NDE elements, only ‘meeting others’ is truly universal in non-Western cultures. Landscapes are nearly universal, but quite variable in their details. Even the OBE does not appear to be a universal NDE element, though it is more common than many of the other elements sought in non-Western NDEs. Encountering a barrier that one cannot cross was equally prevalent. Perhaps most surprising of all is the absence of feelings of peace, a clear tunnel experience, an experience of light, and a life review in almost all of the non-Western NDE reports, given their prominence in the prototypical Western NDE.
Presumably cross-cultural consistency could be explained in terms of either similar neurological events or different encounters with the same afterlife reality. But cross-cultural NDE studies demonstrate that many near-death researchers have simply assumed that the consistency between Western accounts is merely a specific instance of a cross-cultural consistency. For instance, Paul Badham asserts that “What is seen [in NDEs] appears to be cross-cultural, but how it is named depends on the religious or non-religious background of the believer” (Badham 14). Though no prototypical Western NDEs are evident among his Western and non-Western medieval afterlife narratives, James McClenon argues that what is at “issue between ‘believers’ and ‘skeptics’ is not whether common elements exist cross-culturally,” but whether that alleged fact “supports belief in life after death…. [or whether] commonalities within NDEs are produced by physiological factors associated with death trauma” (McClenon, “Folklore” 322). But existing cross-cultural studies suggest that any cross-cultural core consists of a very small number of elements. Thus sociologist Allan Kellehear suggests a very general and rather meager ‘core NDE’ after his survey of non-Western NDE accounts:
In every case discussed, deceased or supernatural beings are encountered. These are often met in another realm…. [which] is a social world not dissimilar to the one the percipient is from. The major difference is that this world is often much more pleasant socially and physically. Clearly, the consistency of these reports suggests that at least these two features of the NDE are indeed cross-cultural (Kellehear 33).
Simply reviewing the existing cross-cultural literature on NDEs led Kellehear to the surprisingly modest conclusion that “the major cross-cultural features of the NDE appear to include encountering other beings and other realms on the brink of death” (34). No other features identified with the prototypical Western NDE appear to be universal.
But if the only truly universal feature of NDEs is encountering other beings in other realms, such little cross-cultural consistency hardly cries out for either a neuroscientific or survivalist explanation. We would expect a real or perceived near-death crisis to produce a sensation of dying congenial to common hallucinations of deceased friends and relatives, religious figures prominent in one’s own culture, and afterlife vistas that—aside from being a better place to live—appear exactly like the world of the living.[28]
Fox suggests, however, that a more specific core NDE can be discerned:
[I]t seems clear that certain motifs do recur within NDErs’ testimonies with some regularity, both cross-culturally and pre-Moody. The presence of some kind of light motif seems very widespread … as does the experience of a period of darkness en route or prior to it (Fox 136).
While these do seem to be recurrent motifs across Western NDE accounts, there is little evidence that prototypical Western NDE motifs appear in non-Western NDEs. NDEs from India, for example, are well-documented in large numbers yet are markedly different from those reported in the West.
Traversing a tunnel or void toward a light is absent from most known non-Western NDE accounts. In fact, given Fox’s assertion that a darkness and light motif is prominent cross-culturally, it is notable that Kellehear (who himself suggests that darkness may be cross-cultural) did not include categories for either ‘darkness’ or ‘light’ in his “Summary of Non-Western NDE Features” table (Kellehear 32).
Since far more differences than similarities have been found between Western and non-Western accounts, the commonalities between different Western NDEs require a special explanation. What could possibly explain consistency between Western accounts but not cross-cultural consistency?
Here a sociological explanation is called for rather than a neuroscientific or survivalist one. The most obvious suggestion is that the widespread dissemination of Raymond Moody’s depiction of NDEs in his 1975 Life After Life produced consistency across Western NDE accounts. Selection bias (omitting incongruent reports) and interviewer bias (asking leading questions) might then account for the consistency between Moody’s reports. (See Fox 199 for a discussion of Moody’s admission of leading subjects on in his Life After Life study.)
But Fox has revealed pre-Moody NDEs from the Religious Experience Research Centre (RERC) archives, which contain over 6000 reports of religious experiences from 1925 to present (Fox 243-44). For instance, RERC account 2733 was written in August 1971 (before Moody had even coined the term ‘near-death experience’) and refers to traveling down a long, whirling black tunnel toward a bright light at the end (Fox 118). At the end of the tunnel the woman reported floating in a warm golden mist in bliss and faces coming out of the mist, smiling, then fading away. The experience ended with ‘waking up’ being slapped by a doctor hard on both sides of the face. (This NDE had occurred just after giving birth; no OBE was reported).
The evidence for consistency between Western NDEs is not limited to this single pre-Moody case from the RERC archives. Similar cases are scattered throughout the literature. An NDE reported by J. W. Haddock in 1851 featured an OBE and life review (Crookall 86). An 1889 NDE reported by Frederic W. H. Myers included an OBE and encountering a dark cloud, a dark pathway, other beings, and a border (Kelly, Greyson, and Kelly 371). In 1935 G. B. Kirkland reported his own NDE, which included an OBE, life review, traveling through “a long tunnel” with a “tiny speck of light at the far end,” seeing others traveling through the tunnel, encountering an uncrossable barrier, then finally returning to his body (Crookall 89). And in 1970 an ineffable NDE marked by clarity of thought included an OBE, “travelling at great speed” sitting on something, noticing a “perfectly rectangular” but porous “pure white cloud-like substance” on an intercept course, and quite pleasantly “floating in a bright, pale yellow light” before ultimately regaining consciousness (MacMillan and Brown 889-890).
Moreover, at about the same time that Moody had published Life After Life in 1975, German minister Johann Christophe Hampe had been independently collecting NDE accounts from psychical research literature and the testimonies of mountain-climbing fall survivors (Fox 55). His German work was translated into English as To Die is Gain in 1979 (Fox 55). Unlike Moody’s accounts, Hampe’s collection included ‘return trips’ back through tunnels, did not include ringing noises, and rarely included encounters with deceased relatives (58-61). Nevertheless, Hampe independently found many prototypical Western NDE features: the realism of the experience, lucid thought during it, OBEs, tunnel experiences, experiences of light, life reviews, and transformations (61).
Finally, a study of the influence of Moody’s model on American and British NDE accounts compared 24 reports of NDEs collected before 1975 with 24 demographic- and situation-matched post-1975 NDE accounts. If familiarity with the depiction of NDEs found in Life After Life had generated widespread consistency between Western NDE accounts, one would expect post-1975 accounts to “include higher frequencies of features included in Moody’s synopsis than do [pre-1975] accounts” (Athappily, Greyson, and Stevenson 219). However, a systematic comparison found no statistically significant difference in the frequency of reports of 14 of Moody’s 15 characteristic NDE features, with only “reports of a tunnel … significantly more common in NDEs reported after 1975 than before” (220).
The discovery of major elements of the prototypical Western NDE in pre-Moody NDE accounts thus rules out Moody’s depiction of NDEs or that of subsequent researchers as the basis of the consistency between different Western NDE accounts. Nevertheless, we should be clear about the differences, even as we acknowledge the commonalities, as Kellehear wisely cautions:
[T]he full image of the NDE is an artifact of the composite picture put together by Moody and repeated endlessly in the NDE literature. Few people actually experience all of these images…. In Ring’s study of clinical NDEs, for example, 60 percent of NDErs experienced a sensation of peace but only 23 percent “entered a darkness” and only 10 percent experienced supernatural scenes. People who are bereaved are probably more likely than NDErs to see deceased relatives or friends….
Our understanding of the NDE has been shaped not by the diversity of NDEs but by a collective portrayal of features seldom occurring all together but immortalized by Moody’s medical vignette (Kellehear 162).
Kellehear points out that about 66% of widows and 75% of parents who lose children experience bereavement hallucinations where their lost loved ones are briefly seen or heard. By contrast, in a recent prospective study where NDErs were interviewed within a week of their experiences, only about one-third (32%) of those who had NDEs reported meeting deceased persons. Even fewer—about a quarter (24%)—reported OBEs. In fact, only two of the ten tabulated elements were found in half or more of the NDErs: positive emotions (56%) and an awareness of being dead (50%) (van Lommel et al. 2041). Thus even the sort of imagery that we would expect to find in hallucinations near death is not nearly as common as our image of the prototypical Western NDE suggests.
Moreover, discrepancies between different researchers’ accounts of the order of NDE elements—whether an OBE is directly followed by a tunnel experience or instead by otherworldly scenes, for instance—is an artifact of trying to “create a pattern out of the welter of various tunnels and paths, lights and presences, gardens and edifices” (Zaleski, “Otherworldly” 123). In other words, in order to portray different NDEs as following a common blueprint, researchers have extracted features from several different NDE accounts from the West and put them back together into one coherent (but artificial) story where the stages of the NDE are clearly defined and follow a “developmental sequence” (123). Nevertheless, there is little doubt that Western NDEs really are “patterned phenomena” marked by similar elements even if “all [of] these stages are not perceived by everyone and … are not necessarily consecutive levels of experience” (Lindley, Bryan, and Conley 105). Moreover, the clichéd commonalities between dreams—dreams of falling or flying, for instance—do not seem nearly as similar between individuals as NDEs do.
With that caveat duly noted, we must return to our original question: How do we explain the consistency between Western NDE accounts? Perhaps Western NDE motifs are found in some part of the Western cultural background other than the NDE literature since Moody. But then one is nagged by a poignant issue raised by Fox:
[I]n the cases where NDEs with classic features such as tunnels and lights are reported, we might wish to question where NDErs actually derive their cultural-linguistic NDE pattern from…. For it is clear that such experiences, complete with recurring motifs such as traversing a period of darkness towards a light, do not represent part of any of the religious traditions of the West (Fox 117).
Specific NDE motifs certainly are absent from the standard depictions of the afterlife provided by Western religious traditions. But Irwin carried out a systematic survey of Western stereotypes of the afterlife to test the hypothesis that NDE motifs derive from social conditioning (Irwin, “Images” 2). Irwin puts that hypothesis as follows: “[I]n a situation of sudden confrontation with death people might draw upon their common cultural heritage to generate comparatively uniform hallucinatory images about a state of existence that is independent of the physical body” (1). Irwin first considers the biblical depiction of Heaven offered in Revelation 21, but quickly notes that biblical sources not only fail to account for the uniformity of Western NDE motifs, but are actually at variance with such motifs:
The difficulty here is that the biblical account is somewhat at odds with the descriptions of the afterlife realm given by subjects of the NDE…. [T]he general public would be well aware of [the biblical] representation of heaven as a city of buildings and streets of pure gold and a surrounding high wall with [pearly] gates. In the NDE on the other hand, the post-mortem realm commonly is reported to comprise a pastoral setting, one with rolling green hills, trees, flowers, perhaps a stream and a blue sky above (Irwin, “Images” 1-2).
As Irwin notes, prima facie “this disparity does not sit well with the view that the near-death experient’s image of the afterlife springs largely from social conditioning” (2). However, he cautions that such biblical imagery does indeed feature in some NDE reports, but more importantly, it is questionable “that the portrayal of heaven in Revelation 21 forms the popular stereotypical image [of the afterlife] in our culture” (2).
Consequently, Irwin set out to determine the most common Western visions of the afterlife by administering a questionnaire survey to 96 introductory psychology students at the rural University of New England in Australia. The survey concerned such variables as the appearance, inhabitants, and means of travel of the afterlife, as well as its auditory features (2). He found that (of each questionnaire item) the most common Western images of the afterlife included a cosmic existence simultaneously everywhere and nowhere in the universe (40%), a pastoral scene of “lush green hills, trees, flowers and streams” (30%), and a formless void of pure being (29%) (2, 3). A mere 7% of respondents selected the biblical image, and 9% expected large gardens to figure prominently in the afterlife (3).
Irwin draws three key conclusions on the basis of this data. First, there are several different Western visions of the afterlife, not just one. Second, the biblical image of Heaven—though widely known—is not widely held, and thus sociological sources of NDE motifs “can not be denied on the grounds that the account of the afterlife in NDEs fails to correspond to the biblical representation” (3). Finally, the image of the afterlife as a pastoral scene—an image often represented in NDEs—is quite commonplace, even though respondents’ questionnaire answers indicate that “the pastoral stereotype generally is not based on familiarity with NDEs” [emphasis mine] (3).
Like the image of looking down upon the Earth from the clouds in the afterlife, a pastoral scene appears to have an obscure but clearly Western cultural source independent of NDE reports themselves. And in turn this image—like that of a garden or the pearly gates—appears to have influenced the content of some Western NDE reports. As Irwin notes, religious indoctrination is one possible source for the pastoral image: “the Bible frequently appeals to pastoral metaphors … [and] Sunday School classes often include exposure to pictures of Christ standing in a grassy, sunlit field” (3-4). And the ‘cosmic’ image of the afterlife, which Irwin suggests is “rooted in diverse mystical and non-Christian traditions,” appears to have been represented in a ‘meaningless void’ experience in which a 28-year-old woman reported encountering a small group of jeering circles ‘clicking’ back and forth from black to white, and vice versa, which she later discovered were Taoist yin-yang symbols—a symbol she likely was subconsciously aware of but had consciously forgotten about (Greyson and Bush 102).
One prototypical Western NDE element may be represented by two items in Irwin’s questionnaire (#6 and #7), which combined indicate that a full 57% of respondents anticipated some sort of illuminating light in the afterlife (3). If we combine being “bathed in perpetual sunshine” with being “illuminated by a soft, diffuse light with no apparent source,” respondents anticipated illuminating light more than any other particular item concerning the appearance of the afterlife, and this was the only feature anticipated by a majority of the respondents. Though ‘illuminating light’ may be too vague to be identified with it, an experience of light is a major Western NDE motif—perhaps the most prominent feature of NDEs in the popular imagination.
Though no other NDE elements are evident in Irwin’s survey, OBEs appear to represent the most natural way to imagine what will happen to your soul immediately after the death of the body (as noted in Veridical Paranormal Perception During OBEs? above). Moreover, Heaven—which polls indicate is where the vast majority of people expect to end up after death (Gallup 5)—is explicitly conceived of as a place of bliss and peace. Tunnels might be the most natural representation of transition for Westerners, as Kellehear has argued. And, as is evident in one of the creation accounts in Genesis, light is often associated with what is good in Judeo-Christian tradition, and God is conceived of as perfectly good. It is not much of a leap to associate God with light, and to think that God would be found on the other side of a transition between life and death. Individuals universally expect to meet others in the afterlife, and most contemporary religious traditions posit some sort of postmortem accounting or judgment of one’s actions during earthly life. Consequently, fear of imminent death might produce a neurophysiological state conducive to dissociative hallucinations, hallucinations whose imagery conforms to NDErs’ culturally conditioned (and perhaps subconscious) expectations of what death is like. In that case it would make little sense to posit specific neurophysiological mechanisms for particular elements of the prototypical Western NDE, just as it would make little sense to posit specific mechanisms for dreams of sailing common in sea-faring cultures but rare in landlocked ones.
Interestingly, aside from Hieronymous Bosch’s suggestive 14th-century painting “Ascent in the Empyrean” (which parallels Gustave Doré’s 1868 painting “Vision of the Empyrean,” an illustration of Canto 31 of Dante’s Paradise), there is scant if any evidence of prototypical Western NDE motifs prior to the 19th century. As both Carol Zaleski’s Otherworldly Journeys and the final chapter of Jan N. Bremmer’s The Rise and Fall of the Afterlife make clear, classical and medieval ‘afterlife experience’ motifs are markedly different from those found in contemporary NDEs. The legend of Er concluding the final book of Plato’s Republic is often cited as the oldest recorded NDE, but like all of Plato’s dialogues, it is entirely fictional, and in any case the only prototypical Western NDE motif possibly present is a vague OBE. (And though Er observes others being judged, he does not experience anything like a modern life review in Plato’s story).[29] In medieval accounts “most of the modern elements, such as the feelings of peace, the tunnel, the hovering above the body, the life review, and meetings with deceased relatives, or even brethren, are generally missing” (Bremmer 99-100). Bremmer surmises that contemporary NDE reports reflect a modern Western individualism absent from earlier afterlife accounts, and proposes this as a potential sociological source of prototypical Western NDE motifs:
{kind=link}
{kind=link}
[In contemporary NDE reports] the normal experience seems to be a feeling of being separated from the body by passing through a dark place, often explained as a tunnel…. The description, though, seems typically modern. How many people in earlier periods would have known of a tunnel? Is it pure chance that in India and China the tunnel is absent from NDEs? Does this experience say something about the way we experience deep down the passing through a tunnel and the feeling of relief when we, literally, see the light at the end?…
Unlike classical and medieval visions, the meeting with relatives or close friends is experienced by about half of the nearly-dead. This surely is a reflection of the disappearance of the separate worlds of man and women and the emergence of the nuclear family as the centre of our affection in the course of the last two centuries…. Whereas earlier generations were immediately certain that they had met angels, modern people lack this certainty, unless they are brought up strongly religiously….
[T]he experiencer often sees his life pass by in a moment. This so-called ‘life review’ or ‘life film’ was already noted [by Albert Heim, who published accounts of over 30 mountain-climbing fall survivors in 1892 after his own fall] before modern NDEs…. [and is] non-judgemental…. one more testimony to the disappearance of hell from the modern imagination…. Can it be that the relatively late appearance of reports of the life film have something to do with the development of the diorama and its reinforcement by the train in the nineteenth century, which enabled people to see a fast succession of scenes as they had never been able to do before?…
What do the modern NDEs tells [sic] us about afterlife? In opposition to what has often been suggested, they do not seem to prove the existence of the ‘life everlasting’, but…. [are] a clear reflection of the modern world, where the development of the individual more and more becomes the main goal of life (101-102).
Kellehear notes parallels which could be taken to suggest a possible cultural source for Western NDE imagery other than religious tradition:
The Velveteen Rabbit contains many of the classic images of the NDE. However, it is not unique in this respect. In The Wizard of Oz, for example, Dorothy is transported inside the “tunnel” of a tornado to another place, where she meets the “good witch of the east.” In Alice in Wonderland, Alice begins her adventure by a long fall down a dark rabbit hole. Children’s literature is replete with tunnels, extraordinary beings, life reviews, flying experiences, and tales of reunion (Kellehear 153).
The suggestion that Western NDE motifs might be derived from well-known children’s stories would account for the considerable consistency between Western NDEs in the absence of evidence of significant cross-cultural consistency. However, the similarities between the imagery described in children’s stories and NDE imagery are superficial at best. Moreover, the stories that Kellehear mentions do not concern what to expect when you die. For a sociological explanation, a great deal is still left unexplained. For instance, why would individuals who felt that they were dying derive NDE imagery from children’s stories rather than better-known and more context-appropriate afterlife imagery from Western religious traditions? Thus any suggestion that there is a connection between prototypical Western NDE motifs and imagery from children’s literature seems rather strained. (Note that Kellehear himself denies that the parallels indicate any connection.)
Evidence of substantial consistency between different NDEs in the West but only trivial cross-cultural consistency opens up two avenues for future research: (1) a sociological search for more compelling links between NDE motifs and possible cultural sources within Western tradition; and (2) more anthropological studies of NDEs in a greater variety of non-Western cultures with larger sample sizes. The latter avenue is paramount: If more robust studies confirm the existence of little or no cross-cultural consistency between NDE reports, the need to search for NDE motifs within Western tradition will become more pressing. But if more robust studies establish that specific NDE elements are cross-culturally consistent, searching for a Western source of NDE motifs will become unnecessary, and knowledge of which NDE motifs are universal or at least widespread would provide us with better data to develop and test specific neuroscientific explanations of NDEs.
Given that at least some NDEs are known to be hallucinations, should future cross-cultural studies uncover universal and well-defined NDE elements, such precise and widespread commonalities would be best explained in neuroscientific terms. Alternatively, if extensive studies fail to uncover substantial cross-cultural consistency between NDE accounts, a sociological explanation for solely Western commonalities would be required.
In any case, our best evidence shows that a survivalist explanation will not do. Despite the commonalities, there is considerable variation in the content of different NDEs. While one person actually sees Jesus, another sees the Hindu god Yamaraj. The glossed explanation that different people simply describe or interpret the same experience in different ways—an encounter with the same ‘being of light,’ for instance—does not do justice to the actual NDE reports that have been collected, where Jesus and Yamaraj have very different appearances and functions.
When NDErs provide very different descriptions of their experiences, there is no reason to assume that different NDErs are simply using different labels to describe the same experience. The most straightforward reason why different NDErs would describe their experiences in different ways is because they actually have very different experiences. The standard survivalist explanation—that despite appearances, different NDE reports really are similar—is simply an ad hoc stipulation.
This principle is widely assumed because different people would naturally be expected to report similar experiences if they were traveling to the same afterlife environment. Of course, the greater the diversity between different NDE accounts, the less credible the NDE consistency argument for survival, and thus the greater the pressure to portray different NDE accounts as more consistent than they first appear.
But NDE reports themselves do not support this principle, and often contradict it, even when considering supposedly core elements. Kellehear, for example, suggests that perhaps:
tunnel experiences are not cross-cultural but that a period of darkness may be. This darkness is then subject to culture-specific interpretations: a tunnel for Westerners, subterranean caverns for Melanesians, and so on. NDErs who do not report darkness may not view this aspect of the experience as an important part of their account or narrative…. Why is the frequently reported sensation of traveling through a darkness by Western NDErs so often described as a tunnel experience? (Kellehear 35-36).
But the most straightforward interpretation of apparent diversity is actual diversity: that Westerners actually see tunnels in their experiences, while Melanesians see underground caverns. But since acknowledging actual diversity tends to undermine arguments for survival based on NDE commonalities, it is not surprising that researchers sympathetic to survival after death tend to interpret markedly different NDE reports in terms of the ‘same experience, different descriptions’ principle.
Though he notes the possibility, Kellehear provides no evidence that NDErs actually use different labels to describe the same experience. Consider the proposition that the term ‘tunnel’ is just one of many possible misnomers for a more generic experience of darkness. If an episode of darkness were a cross-cultural element, for instance, then NDErs’ use of the term ‘tunnel’ would typically represent the use of a less-than-ideal descriptor for such an episode. But Kellehear offers no supporting excerpts from open-ended interviews in which, as further details unfold, NDErs’ initial use of the term tunnel clearly refers to an episode of darkness.
After finding several accounts of visiting outer space in the RERC archives, Fox asserted that many NDErs “were found to use the descriptor ‘space’ to describe the episode of darkness” (Fox 265). Soon after he wrote: “The significance of the word ‘space’ to describe the darkness encountered in these experiences will be returned to” (265). Finally, Fox skewed what was actually reported by NDErs by concluding that many of his RERC respondents “describe an encounter with some sort of darkness motif in terms seemingly suggestive of a visit to outer space” (277).
Fox is speaking as if he knows ahead of time what these different people have experienced. But of course assuming that these reports are describing the same thing regardless of what they actually say begs the question, for that is the very issue of contention. Fox asserts that the episode of darkness is what is encountered, but that it is being described as ‘space’—but how does he know that it was not space that was actually encountered? Of course he doesn’t know; he just assumes.
If we look at such NDErs’ actual testimonies, one person reports encountering a tunnel while another reports encountering space. But shouldn’t we take each at his word instead of assuming that both are encountering the same darkness in order to fit our artificial NDE models? Just because space, tunnels, and underground caverns are dark does not mean that astronauts, motorists, and miners are using different terminology to describe traveling to the same place. One wonders just how much consistency is being derived from NDE reports rather than being read into them.
Worse still for the ‘same experience, different descriptions’ principle, many NDErs report encountering tunnels with physical properties, such a being made of bricks. Consider a case reported by Peter and Elizabeth Fenwick:
[T]he tunnel was made of polished metal, jointed and held together with something like rivets…. I felt it should have been more ethereal somehow … My feet felt like lead but as I walked back to life the light threw my shadow on to the floor of the tunnel as I walked away from it (Fenwick and Fenwick 55).
Clearly a case like this could not simply be a description or interpretation of a mere ‘episode of darkness.’ More plausibly, different NDErs experience different things: traveling down tunnels, floating in ‘outer space,’ walking down a road, being caught in a calabash, and so on.
In sum, despite several recurrent and well-defined commonalities across different Western NDEs, very few and only broadly defined commonalities have been found cross-culturally. This is problematic for a survivalist interpretation of NDEs because a substantial cross-cultural core would be expected if different NDErs were literally traveling, by the same means (leaving their bodies) and through the same route (passage through a tunnel or darkness toward a light), to transcendental destinations. Instead, we find a variety of culture-specific NDE templates with only locally well-defined commonalities. This severely undercuts the survivalist argument that NDE commonalities result from different NDErs undergoing the same journey; and in virtue of their common humanity, NDErs would not be expected to take different journeys to different places after death merely because of where and when they lived while on Earth.
Thus there are two ways in which NDE diversity undermines a survivalist interpretation of NDEs. First, arguments for a survivalist interpretation are often premised on purported uniformity across times and cultures. Insofar as the rule seems to be substantial diversity, however, one foundation for a taking a survivalist interpretation of NDEs is eliminated. Second, NDE diversity provides positive grounds for thinking that a survivalist interpretation is likely to be false. Encounters with different transcendental environments might explain starkly different landscape visions, but would not explain different modes of travel to those “otherworlds.”
For instance, if NDEs are transitions to another world initiated by something leaving the body, then all NDEs ought to begin with OBEs. But a substantial portion of prototypical Western NDEs do not include OBEs at all, and non-Western near-death OBE accounts are sporadic. Are NDErs who do not report OBEs simply amnesic about leaving the body, even though NDErs commonly report recalling their NDEs more sharply than any other events in their lives? Why do out-of-body NDEs in the West typically transition quickly from seeing the physical body and its immediate surroundings to another NDE element, while NDErs from Guam evidently “project” thousands of miles away to see relatives living in America? These sorts of questions are awkward for those taking a survivalist interpretation of NDEs.
On a survivalist interpretation, feelings of peace, OBEs, passages through a tunnel or darkness toward a light, and life reviews are initial stages of a transitional experience from this world to the next that should be common to all or most human beings, even if “the next world” in fact consists of multiple “otherworlds.” These initial stages would be expected to be present, by and large, cross-culturally and across historical eras. But these elements are strikingly absent from most extant non-Western NDE accounts.
Even within highly consistent prototypical Western NDEs, there is wide variation in the form that NDErs’ “astral bodies” take: sometimes they are mirror images of the normal physical body, other times they are balls of light or amorphous clouds, and sometimes NDErs do not even perceive having a “secondary body” at all (Irwin, “Introduction” 225; Moody 37). But if NDErs’ secondary bodies were real rather than imaginary, we would expect their described characteristics to be about as uniform as those of different human beings’ normal physical bodies. And though most NDErs describe their out-of-body vision as comparable to normal 180° color vision, some report surprising idiosyncratic traits like 360° “spherical vision” (Ring and Cooper, “Blind” 139) or at-will x-ray vision (Lawrence 125). Though such differences might be explained in terms of extremely variable astral genes or other fanciful constructs, such peculiarities are certainly awkward for a survivalist interpretation of NDEs.
Blackmore makes a similar point concerning tunnel experiences: “The tunnels described [in prototypical Western NDEs] are all different in precise form…. Presumably if there is a ‘real’ tunnel then it should have one form and all the rest must be seen as inaccurate perceptions of that real tunnel” (Blackmore, “Dying” 77). Of course, it may be that there are different passageways for different NDErs, with some taking tunnels and other traversing a dark void; but even granting this, if NDErs were accessing shared realities rather than purely subjective imagery, we would expect more uniformity across accounts than a particular kind of tunnel tailored for each individual NDEr, with some NDErs foregoing traversing any sort of passageway whatsoever.
Since such inconvenient facts for a survivalist interpretation of NDEs could be repeated ad nauseam, I will mention just one other example. Taken literally, the deepest NDEs (e.g., Dannion Brinkley’s NDE) seem to imply a communal afterlife subject to some form of governance. But if NDEs were glimpses of such an afterlife, we would expect to see some sort of pattern in the distribution of pleasant and distressing NDEs. For instance, we might anticipate predominantly altruistic or spiritual individuals fairly consistently reporting pleasant NDEs, while predominantly antisocial or profane individuals tend to report distressing ones. Alternatively, we might anticipate that all NDErs report by and large pleasant NDEs. Or there might be some other conceivable pattern consistent with afterlife governance. In fact, however, altruistic individuals appear to be no less likely to have distressing NDEs than anyone else, and antisocial individuals seem no less likely than others to have pleasant NDEs. Instead, the character of one’s NDE seems to be determined primarily by either “the person’s mindset immediately prior to the experience” or “programming during childhood” (Rommer 196). On any model of a governed afterlife, this distribution appears to be entirely random and difficult to explain; but it is exactly what one would anticipate on a psychophysiological model of NDEs.
Greyson concedes stark cross-cultural variation, but argues that “experiences which conflict with [NDErs’] specific religious and personal expectations of death” challenge the view “that NDEs are products of imagination, constructed from one’s personal and cultural expectations” (Greyson, “Near-Death” 332). However, his argument fails, and in any case a few cases of apparent ‘cultural dissonance’ in NDEs certainly does not outweigh an abundance of evidence for the predominant role of expectation in NDEs from different cultures, such as those from India and Thailand.
Greyson cites the case of the Jewish NDEr Chaim Ralbag, who experienced an unusual cardiac arrest NDE in which he was falling into a dark void a high speed, hovering over a sea of nothingness, then pushing himself back out of the void. As he traveled upward through the void, his surroundings were illuminated, and eventually he saw his body lying on the ground (Abramovitch 177-178). As his NDE progressed, other ‘astral beings’ appeared, more and more by the minute, “all in motion, ever taking on new forms, expanding, revolving, and contracting in their movements, merging and penetrating, passing and affecting one another” (178). He had an experience of light, communicated with another being, and noticed a steep hill above a misty area. While walking toward the hill, he encountered his deceased father and brother, but after his father told him to return to the body before it was “too late,” he experienced intense pain and saw their faces fade away. Next he appeared to be hovering over his body on the ground again, then finally woke up in the recovery room.
Henry Abramovitch, who first reported the case, cites two reasons why he thinks that expectation cannot account for the content of Ralbag’s NDE. First, Ralbag was taught that the biblical Adam would appear to the dying (much as some Christians are taught that St. Peter will appear to them at the Pearly Gates), but this did not happen in his NDE. Second, he was taught that he would face judgment in the afterlife, but had no life review (Abramovitch 182-183). That an individual’s visions of the afterlife do not exactly mirror what he was taught, however, hardly requires an encounter with the afterlife to explain it.
The real issue is whether such experiences conflict with an individual’s personal expectations. And there are two further issues here. First, what a person consciously claims to expect of the afterlife says nothing of his subconscious expectations, which would surely come into play during an altered state of consciousness like an NDE. Think of how many dreams that you can recall whose content has nothing to do with what you consciously think about during your waking hours. Second, many individuals do not simply accept whatever dogma was taught to them in childhood, but grow to elaborate upon, modify, or reject what they were taught, subject to influence from personal inclinations and a variety of alternative traditions, even some only vaguely known (e.g., Westerners’ understanding of Eastern beliefs like reincarnation).
Murphy found clear evidence of this in an NDE reported by the Chinese-Thai Kodien. During his NDE,
He noticed that some groups [of deceased people] had food and water, while others had only piles of ash…. He asked for something to eat. Kodien asked “Is this your food?” His friend said “Yes, but you can’t eat any of it because it doesn’t belong to you…. Your food is over there.” Kodien’s friend pointed to a pile of ash…. His friend said that those who made merit by donating food to the monks during their lives would have food [in the afterlife], while those who only helped their own ancestors (by burning joss-paper replicas of food according to Chinese tradition) would only have piles of ash. Kodien realized that his friend was suggesting that he create merit according to the Thai custom, but during his life he had not believed in the practice. He had thought that the Chinese forms of religious observance were better, and had only made joss-paper offerings (Murphy, “Thailand” 168-169).
Here an NDE is shaped almost entirely by cultural influences, yet the NDEr experiences something contrary to his conscious beliefs. But this ‘cultural dissonance’ does not imply that this NDE was not expectation-driven, as Murphy explains:
His NDE seemed to reveal that he was actually more drawn to the Thai ways of creating merit than to those of his own family and subculture…. [This] suggests that it is not culture alone that determines NDE phenomenology. Rather, NDEs may be determined more by one’s expectations concerning what death will be like, even when those expectations are held subconsciously or are influenced by more than one culture (169).
A much more impressive case of cultural dissonance would be finding a sheltered Midwestern boy who has never had contact with anyone from Asia or Southeast Asia, but nevertheless reports encountering Yamatoots during an NDE.
Greyson goes on to argue that “children too young to have received substantial cultural and religious conditioning about death report the same kinds of [NDEs] as do adults” (Greyson, “Near-Death” 332). But how young is “too young” for a child to be affected by cultural conditioning? Children younger than 3 years old clearly learn concepts from sources as ubiquitous as television advertising. Moreover, how confident can we be that children’s NDE reports have not been contaminated by parental influence or interviewer feedback? Children are particularly susceptible to influence from authority figures and typically have much richer imaginative lives than adults. The risk of direct contamination from parents or researchers could be minimized by closing the gap between the time of the NDE itself and when it is reported, but such crucial evaluative information is rarely published.
Random Memories
Another feature which suggests that NDEs are not perceptions of an external afterlife reality is the random nature of the life review. The glamorized picture provided by Moody’s artificial composite NDE portrays the life review as a personally significant ‘learning experience’ where one is either judged by other beings or by oneself for past wrongdoings. While this characterization does fit some cases—and indeed is found even in people who face life-threatening danger but never really come close to death (e.g., see Blackmore 183)—the frequency of ‘learning experience’ type life reviews appears to have been exaggerated by some near-death researchers. At least one researcher sympathetic to the survival hypothesis has found that most near-death life reviews do not fit this pattern.
Several researchers have found that life reviews are generally rare in NDEs. The Fenwicks found recalled memories in only 15% of their 350-person sample. Though their retrospective reports were not randomly collected, a similar incidence (13%) of life reviews among NDErs was subsequently found in a more representative prospective study of NDE incidence and transformation (van Lommel et al. 2041). Thus, in the Fenwicks’ sample the incidence of recalled memories is comparable to that of encounters with living persons. Their 350-person survey is one of the largest retrospective surveys of NDEs ever compiled. (Retrospective surveys are those done well after the experiences occurred.) Their findings contrast sharply with portrayals of the life review popularized by Moody and others.
(1) For example, the Fenwicks found only one person in their sample of 350 NDErs who had recalled a ‘learning experience’-type life review during his NDE. Here is the sort of life review typically found in their sample:
The seconds that went by as the car was turning [over repeatedly] for me seemed an eternity…. Then, suddenly, I became detached from my worldly body—I was seeing my life flash before me, recalling my family, friends, the man on the bus, the lady in the shop—and feeling confused but happy. At this time I was in a tunnel-like black space. Just beyond a light was glowing invitingly (Fenwick and Fenwick 57).
This is hardly a description of the ‘morality play’ style life review we’ve come to expect from the popularized picture of the NDE provided by some near-death researchers. In fact, Blackmore acknowledges that a physiological explanation of such a coherent life review would appear implausible to many:
[In the NDE] there is generalized amplification of [brain] activity and so lots of memories can be invoked all at once or in sequence. You might then object that such generalized activity could only produce random memories and not the connected and meaningful experiences of the near-death life review (Blackmore, “Dying” 216).
But, remarkably, the Fenwicks almost always found random memories in their sample of life reviews:
Although 15 per cent of the people we questioned said that scenes or memories from the past came back to them during the [near-death] experience, most of these were simply fragments of memory, sometimes quite random memories. Only about half said the memories that came back to them were [even] ‘significant’ (Fenwick and Fenwick 116).
The Fenwicks conclude that near-death life reviews “are not necessarily particularly significant memories. They seem just as likely to be random moments plucked haphazardly from memory, trivial events or people or places” (118).
The Fenwicks’ findings imply that the memories recalled during NDEs are barely distinguishable from the flashbacks of temporal lobe seizures. While this isn’t flatly inconsistent with a survivalist interpretation, it is clearly readily explicable on physiological models of the NDE, making a survivalist interpretation unnecessary.
Is the Temporal Lobe Implicated in NDEs?
As Christopher C. French points out, there have long been indications that the temporal lobe is implicated in NDEs:
The temporal lobe is almost certain to be involved in NDEs, given that both damage to and direct cortical stimulation of this area are known to produce a number of experiences corresponding to those of the NDE, including OBEs, hallucinations, and memory flashbacks. It is worth noting that both the temporal lobes and the limbic system are sensitive to anoxia, and that release of endorphins lowers the seizure threshold in the temporal lobes and the limbic system (French 357).
That OBEs could be induced by electrical stimulation of the temporal lobe has been known at least since 1941 (Tong 104-105). While electrically stimulated OBEs may be phenomenologically distinct from spontaneous ones, realistic, continuous, stable, ecstatic, and otherwise apparently indistinguishable OBEs have been reported accompanying temporal lobe seizures (Devinsky et al. 1081-1086; Vuilleumier et al. 116). Like spontaneous cases, OBEs evoked by temporal lobe seizures often incorporate accurate reconstructions of events surrounding OBErs’ bodies (e.g., case 7 and patients 33, 39, and 40 in Devinsky et al. 1082, 1086, respectively; and in a single epileptic who had recurring OBEs for over 10 years in Vuilleumier et al. 116), as well as occasional small but significant out-of-body discrepancies (e.g., case 4 in Devinsky et al. 1081, where an epileptic OBEr would see his body in the correct clothing but with combed hair even when he knew it to be uncombed beforehand).
Additionally, French notes that peace or euphoria and mystical feelings “are often reported by temporal lobe epileptics just prior to a seizure,” quoting a patient stating that nonepileptics “can’t imagine the happiness that we epileptics feel during the second before our attack” (French 358). Some epileptics “even see apparitions of dead friends and relatives” (Blackmore, “Dying” 206). So several NDE elements—including feelings of peace, OBEs, a sense of timelessness, life reviews, and encounters with others—suggest a role for the temporal lobe in the phenomenology of the experience.
Willoughby B. Britton and Richard R. Bootzin offer similar observations implicating the temporal lobe in NDEs. First, “electrical stimulation of the temporal lobe and seizures in temporal lobe epileptics can evoke similar mystical experiences.” Second, “acute stress or hypoxia during a life-threatening event may hypersensitize neurons and lower seizure thresholds, especially in the temporal lobe.” Finally, both NDErs and temporal lobe epileptics “share the tendency to be transformed by their experiences and take on new spiritually oriented interests and values” (Britton and Bootzin 254).
Against such observations, Greyson argues that “key features of NDEs … have not in fact been reported either in clinical seizures or in electrical stimulation of [temporal lobe] brain structures” (Greyson, “Near-Death” 335). But contrary to Greyson, the observations above illustrate that many key features of NDEs are found in such circumstances. Moreover, those advocating a role for the temporal lobe in the production of NDEs are not claiming that NDEs ‘just are’ temporal lobe seizures, but rather that similar temporal lobe activity, in conjunction with other activity in a dying brain, is implicated in NDEs (Blackmore, “Dying” 215-216). That temporal lobe stimulations or seizures do not produce every prototypical Western NDE element, or that they sometimes produce phenomenologically distinct experiences, does not indicate that the temporal lobe is immaterial to producing NDEs. For instance, damage to the temporal lobe can produce visual agnosia, the inability to recognize familiar objects despite clear vision, but temporal lobe stimulations or seizures cannot, simply because the former has more profound consequences for overall brain functioning than the latter.
Fox has uncovered further evidence that temporal lobe activity may bring about NDEs. He notes that when he examined complete NDE accounts from the RERC archives, rather than the incomplete extracts published by major near-death researchers, he found signs of temporal lobe epilepsy in a significant number of NDErs. In particular, he found signs of hypergraphia, a compulsion to write extensively about spiritual realities. In one case from the RERC archives, for example, a man reported an OBE, a tunnel experience, encounters with deceased relatives, and a life review, followed by 11 pages of speculative hypergraphic testimony about the meaning of life, the purpose of existence, the soul, and the beginning of the universe (Fox 161). Fox concludes that:
hypergraphia has long been recognized as a symptom of temporal lobe epilepsy. Whilst the presence of hypergraphia within NDErs’ reports has been hidden from view often because of the editing of accounts carried out by near-death researchers themselves, an examination of original accounts … reveals that hypergraphia is a significant feature of a significant number of accounts (161).
Plausibly, OBErs and NDErs have greater dissociative tendencies than control groups because they are predisposed to dissociate. Dissociative tendencies, in turn, are correlated with nonpathological temporal lobe instability as measured by various temporal lobe signs (Richards and Persinger 1139). This suggests that those with greater temporal lobe instability may be more prone to have NDEs than others—a hypothesis which is testable in any number of ways, one of which is suggested by Blackmore, who predicts “that the highest level of temporal lobe signs would be found in those who have NDEs when not medically near death, next highest in those who have NDEs near death and lowest in those who come close to death but have no NDE” (Blackmore, “Dying” 218). Though circumstantial, evidence of temporal lobe instability among NDErs comes from findings that NDErs report undergoing more mystical experiences than average prior to their NDEs (Greyson and Stevenson 1195), and having more OBEs and ‘psychic’ experiences than non-NDErs (Kohr 160; Makarec and Persinger 838). Greyson and Stevenson also found that perceptions of time distortion were significantly correlated with ecstatic feelings during NDEs (Greyson and Stevenson 1195). These elements are associated with temporal lobe instability in non-NDE contexts, and there is no other apparent reason for them to be correlated in NDEs.
Recently, Britton and Bootzin carried out a more systematic investigation of the relationship between NDEs and the temporal lobe, comparing their NDE group to a control group. Their NDE group included subjects who had experienced “life-threatening physical distress as the result of an accident or other injury and [received] a minimum score of 7 on the [Greyson] Near-Death Experience Scale” (Britton and Bootzin 254). Their non-NDE control group consisted of age- and gender-matched individuals who had not come close to death and who had scored below 7 on the Greyson NDE Scale. Despite having used a less-than-ideal control group, the authors provide convincing evidence that their findings confirm a role for the temporal lobe in the production of NDEs. These findings include:
- NDErs were about four times as likely to have temporal lobe epileptiform EEG activity during sleep than non-NDErs (255).
- NDErs “reported significantly more temporal lobe symptoms” than non-NDErs, such as “frequent anomalous experiences, sleepwalking, olfactory hypersensitivity, and hypergraphia,” and scored significantly higher than non-NDErs on a measure of epileptic signs typical of temporal lobe activity, including “feelings of intense personal significance and unusual olfactory, auditory, or visual perceptual experiences” (255).
- Not only did NDErs take longer to enter REM sleep than non-NDErs (255), but there was a positive correlation between the depth of a subject’s NDE (as measured by the Greyson NDE Scale) and the delay in REM sleep onset, so that the deeper the NDE, the greater the delay in the onset of REM sleep (256).
- NDErs scored significantly higher on measures of coping skills than non-NDErs (256).
- NDErs scored marginally higher than non-NDErs on the Dissociative Experiences Scale (DES), and significantly higher than non-NDErs on the Amnestic subscale of the DES—the latter of which measures things like not remembering how you arrived at your destination. These findings indicate that NDErs show a greater (but nonpathological) tendency to dissociate than non-NDErs (256).
Some might object that Britton and Bootzin’s findings are equivocal because they used the second-best control group available: non-NDErs. Indeed, their findings would have been more decisive if they had used the ideal control group: non-NDErs who came close to death. As they concede, it is possible that the general trauma of coming close to death—not whether subjects had an NDE—is what accounts for the differences between the two groups. However, they anticipate this objection and provide substantial evidence that generalized trauma does not account for the differences between the two groups, implying that it is the occurrence of the NDE itself that is correlated with these differences (257). This correlation, in turn, implies that certain people are physiologically prone to have NDEs, whereas others are not.
First, the authors note that there was a significant correlation between Greyson NDE Scale scores and both the temporal lobe epileptiform EEG activity and the delayed onset of REM sleep; but these characteristics were not correlated with any of the collected scores for measures of trauma (257). If the trauma of coming close to death had caused the epileptiform EEGs in the NDE group, then those EEGs should have been correlated “with trauma-related factors to a similar degree,” but they were not. Instead, left temporal lobe activity was more highly correlated with Greyson NDE Scale scores than with scores on measurements of posttraumatic stress disorder or dissociative disorders, or with a history of head trauma (256-257). Second, although their NDE group included a few subjects with head trauma, a regression analysis found that head trauma was unrelated to epileptiform EEG activity (257). Additionally, the general incidence of epileptiform EEG activity in those who become unconscious without head trauma is 5.7%, as compared to the significantly higher rate of 22% in Britton and Bootzin’s NDE group (257). Third, that the epileptiform EEG activity in the NDE group was almost entirely limited to the left temporal lobe is atypical of any other group, implying that NDErs are neurophysiologically unique (257-258). Finally, unlike typical trauma survivors, the physiological differences between the NDE group and the non-NDE control group “were not associated with negative stress reactions” but “instead with positive coping styles” (258). A preponderance of the evidence, then, implicates the temporal lobe in the production of NDEs. Britton and Bootzin conclude:
Taken together, the temporal lobe, sleep, and psychological findings are not consistent with posttraumatic symptomatology. However, they may be indicative of a preexisting condition that predisposes individuals to unusual reactions to acute stress. These data are the first objective evidence of neurophysiological differences in near-death experiencers (258).
Threshold Crossings: Returns from the Point of No Return
In some NDEs the experiencer encounters a barrier or divide felt to be a threshold between life and death—a fence, gate, door, river, line, mist, even ‘the light at the end of the tunnel’ itself. Kenneth Ring even found a case where a woman ferried across the River Styx during her NDE (Zaleski, “Otherworldly” 149). Those NDErs who encounter some sort of barrier or threshold typically state that they are told or otherwise somehow know that if they cross the threshold, they cannot turn back and return to life. This feature of some NDEs has prompted the Fenwicks to ask: “If the whole [near-death] experience is psychological, then why hasn’t someone crossed the barrier and come back to tell the tale?” (Fenwick and Fenwick 111).
The Fenwicks speculate that the answer may be that we cannot psychologically form an image of our own deaths. This may be why we never ‘die’ in our dreams, for example (111). But the explanation that NDEs are literally glimpses of an afterlife is flatly inconsistent with features of some of the very NDEs that the Fenwicks have found. A better answer than either of these possibilities, however, is that some NDErs have indeed crossed a divide thought to be a point of no return, or otherwise decided to stay in the ‘NDE world’ when given a choice, and yet still returned to life.
(1) The Fenwicks themselves presented the case of the NDEr cited earlier who was beckoned to board a blue train ‘into the afterlife’ and did so, though his experience ended with the sensation of being resuscitated. Didn’t boarding the blue train seem a lot like crossing a ‘point of no return’? But if this NDEr had really crossed a final threshold in another realm, why did he eventually ‘come to’ on the deck of the frigate?
The NDEr reported that the passengers had beckoned him to board the train, implying that doing so would be a significant decision to cross a point of no return. Moody, for example, reports the case of a nurse giving birth for the first time who found herself sailing across a large waterway being beckoned by dead relatives to join them. The nurse reported immediately telling them that she wasn’t ready to die, implying that she automatically knew crossing over to the shore on the other side of the waterway would be going past a point of no return (Blackmore, “Dying” 193). In the Fenwicks’ case the NDEr actually did board the blue train—he did appear to cross a point of no return—yet still returned to tell the tale anyway.
This NDEr didn’t describe boarding the train explicitly as crossing a point of no return, but it certainly seems reminiscent of the one-way boat trip across a river felt to be a point of no return described by other NDErs (e.g., Moody’s case above and the childhood NDE reported by Morse where living playmates are seen on the other side of a river).
Ultimately, even the Fenwicks concede this:
David Whitmarsh meets no barrier. When people on the train beckoned to him he was actually able to go aboard. Nothing seemed to be holding him back or preventing him from boarding. One feels that David was well on his way [to the afterlife?] when resuscitation intervened (Fenwick and Fenwick 155-156).
But if his double had detached from his normal physical body long ago and was well on its way to ‘the other side,’ how could he have felt his resuscitation, and how could it have brought him back into his body? We would expect these features if he had ‘been inside’ his body the entire time and bodily sensations eventually became part of his hallucination.
(2) Serdahely reports a case where an NDEr explicitly says she crossed a barrier between life and death and yet still was restored to life:
One of the three [NDErs told to return] was instructed apparently by a deceased grandmother not to cross a line in front of her. The OBEr did cross the line, at which point the grandmother said, ‘I told you not to cross the line.’ The older woman ‘got right in [her] face’ and said, ‘You are to go back now!’ (Serdahely, “Variations” 191).
(3) After undergoing a panoramic life review during his NDE in 1978, Tom Sawyer was both given a choice and decided not to return to life by entering the light at the end of the tunnel, but was nevertheless ‘returned’ to life:
I was given a choice. I could return to normal life or become part of this light…. I chose to stay and become part of that light. I then had the feeling of going through the tunnel in reverse, and I slammed back down into my body (Harris and Bascom 129).
If NDEs are brain-generated hallucinations, nothing would seem to prevent experiences where NDErs decide not to return to life, or cross ‘a point of no return,’ but find themselves restored to life anyway; and in these cases we find exactly that.
Who Makes the Decision to Return?
Blackmore reports being impressed by the fact that so many different NDErs are uncertain about just who made the decision for them to return to life (Blackmore, “Dying” 230). Moody also found that many of his Life After Life subjects were unsure of how or why they returned to life:
The accounts I have collected present an extremely varied picture when it comes to the question of the mode of return to physical life and of why the return took place. Most simply say that they do not know how or why they returned, or that they can only make guesses (Moody 79).
Many NDErs appear to be reaching, after the fact, for some sort of explanation for why they returned to life, when none is apparent in the NDE itself. Some of the NDErs in the Fenwicks’ sample openly wondered why they were ‘sent back,’ for they found no reason to continue living; after their NDEs they continued working menial jobs, for instance.
Blackmore’s conclusion about the ‘decision to return’ is poignant here:
So who does make the choice to return to life?… There does not seem to be a clear answer. It could be that there are genuine choices available to some NDErs and not others; that some can really make a choice and others have it made for them. To me this seems unlikely. It seems more likely that they are all trying, and with difficulty, to describe something that is not either their own choice, nor someone else’s choice (Blackmore, “Dying” 232).
When you wake up from a dream, do you suppose that one of your dream characters decided to wake you up? Or that you woke up because in this dream world you yourself made a decision to wake up? Or does your dream end simply because your brain is no longer in the right electrochemical state for the dream to continue? I think this last explanation is the best one, even in lucid dreams where the dreamer has some control over dream content. Occasionally, a dream character may even pronounce that a dream is coming to an end, or a lucid dreamer may seem to have the ability to end a dream. In such cases, it is likely that a physiological change, from an external sound to a change in one’s wakefulness, causes dream content to coincide with actually waking up.
A similar explanation seems plausible for the so-called ‘decision to return’ in near-death experiences, where NDErs often seem to struggle with trying to figure out who made the decision. In their study van Lommel and colleagues found that only 5 out of the total 62 NDErs (8%) even reported encountering a border between life and death; this was the least common NDE element found (van Lommel et al. 2041). Most NDErs simply find themselves ‘back in their bodies’ with no idea of how they transitioned back to normal consciousness, just as we would expect if the physiological conditions necessary to maintain hallucinations had disappeared.
Hallucinatory Imagery
(1) One feature rarely noted in popular accounts of NDEs is hallucinatory imagery seen in the experience. For example, when one man was accidentally electrocuted, he encountered a mythological creature during an NDE:
The next thing I remember, there was a cloud and a male, related to Jesus, ’cause he looked like the pictures of Jesus. He was in this chariot type [thing]… the torso was a horse, everything above the torso was a man with wings; sort of like a Pegasus except instead of a horse’s head it was a man… and he was beckoning to me… and I kept backing up… I remember telling him no, I had too many things to do and there was no way I could go now. Then the clouds sort of filled over and as it filled over I hear Him say, “O.K.!” [ellipses original] (Lindley, Bryan, and Conley 116).
Perhaps a centaur with the head of a man resembling depictions of Jesus and the body of a winged horse is waiting to guide us into the afterlife in a chariot; but the fantastic quality of this and other NDEs strongly suggests that NDEs are hallucinations.[30]
(2) In one of the Fenwicks’ cases a man who had a heart attack while in the hospital reported having an out-of-body experience where he was flying as a ‘junior member’ in a formation of swans he’d seen earlier; while flying the landscape below him appeared to quickly regress backward in time. He ‘saw’ a cathedral being built and men in medieval garb sailing on large lakes (Fenwick and Fenwick 128). Such fantastic imagery suggests that this NDE was a hallucination; it seems absurd, for example, to seriously ask whether the swans he saw earlier were really flying with him backward in time.
(3) In his 1982 study Recollections of Death, Michael Sabom found a rather bizarre case which also suggests that NDEs are hallucinations. In case I-21, Sabom’s subject reported feelings of peace, bodily separation, traveling through a dark void, and encountering a light after a heart attack (Sabom, “Recollections” 197, 204, 206). The NDEr also encountered “four unknown nurses” who interrogated him “about possible ‘subversive activities'” (210).
Like Morse and the Fenwicks, Sabom also found encounters with living persons during NDEs. In case I-8, a woman encountered her living children in her NDE but didn’t communicate with them (53-54). Though no other details are published in the study, case I-24 includes an encounter with a living granddaughter (210).
(4) From time to time Western NDE reports describe the world encountered during NDEs in terms that are uncomfortably familiar, mirroring the transient technological advances of the present-day living. After being resuscitated from a heart attack, for instance, one woman reported “watching details of her life being noted down … [by] a computer” (Zaleski, “Otherworldly” 129).
(5) In a case from the RERC archives (RERC account 3583), a hospitalized woman had an unusual NDE that started as an out-of-body experience. After moving through the ceiling, instead of seeing her Australian hospital from above, she reported finding herself on a Russian battlefield “piled with dead men,” Russian tanks, and machines. Then she found herself in a hospital run by nuns where a screaming woman giving birth was silenced by nuns “stuffing a pillow on to her head to stop her cries” (Fox 283). Next she reported being back in her hospital bed and feeling ill, wondering if her NDE was a hallucination caused by medication.
(6) In another of the Fenwicks’ cases, a woman had an NDE during a particularly bad case of the flu. She reported having an out-of-body experience, floating up to a green field containing a large tree “with a brilliant white light on top,” and meeting her deceased father. When her father waved her away, she returned to her body, opened her eyes, and saw that “there was steam coming out of my hands” (Fenwick and Fenwick 29). The Fenwicks concede that the steam was one of the “hallucinatory qualities” of her experience and speculate that her high temperature might have produced it (30).[31]
(7) Sometimes a prototypical NDE will incorporate terrifying hallucinatory features. After skidding on black ice, wrecking his car, and pulling out other passengers, a student collapsed and had to be resuscitated at the scene of the accident. While on life support in the hospital, he had two heart attacks and reported the following distressing NDE:
I was in a tunnel and sensed I was travelling towards a brightish light hidden behind a bend in the cave…. I felt I was simply floating—I did not have the use of my arms or legs at all….
As I passed round the bend in the cave I saw a giant Dracula-type of mouth opening. I say ‘Dracula’ because there were two monstrous fangs with blood dribbling off them…. I gained the instant impression that if I proceeded towards the mouth, it would shut and the teeth would slice me in two and kill me (Fenwick and Fenwick 190-191).
The student woke up screaming for his mother, was comforted by her, was given a tranquillizer, and then slept for a few hours.
(8) Morse provides an NDE account from a boy who was 4 years old when he almost drowned after the car he was in skidded on ice and plunged to the bottom of a river. The boy reported accidentally going to ‘animal heaven’ and speaking to a bee after losing consciousness:
I went into a huge noodle…. It wasn’t like a spiral noodle, but it was very straight, like a tunnel…. When I told my mom about nearly dying, I told her it was a noodle, but now I am thinking that it must have been a tunnel, because it had a rainbow in it….
I was being pushed along by a wind, and I could kind of float. I saw two small tunnels in front of me. One of them was animal heaven and the other one was the human heaven. First I went into the animal heaven. There were lots of flowers and there was a bee. The bee was talking to me and we were both smelling flowers. The bee was very nice and brought me bread and honey because I was really hungry (Morse and Perry, “Parting” 4).
Next he reports going to ‘human heaven’—which he describes as a ‘regular old castle,’ encountering his dead grandmother, hearing loud music, then finally simply ‘waking up’ in the hospital surrounded by nurses (4-5).
Interpreted at face value as evidence for survival, this NDE implies that life after death is not limited to human beings, mammals, or even vertebrates. While we cannot rule out the possibility that human beings may encounter insects in the afterlife and have discussions with them, it seems more likely that this childhood NDE was a hallucination. It also seems unlikely that one’s double would feel a bodily sensation like hunger in the afterlife which could only be satisfied by astral nourishment.
(9) In another case a childhood NDE was also triggered by nearly drowning. In this NDE an 8-year-old girl encounters seven other children, a butterfly, and a deer:
I was in a garden, right behind a bush…. [T]here was this one, big, large tree and there were children playing a game [ring-around-the-rosey]…. I saw a bunch of flowers, there was a butterfly and a deer next to me who I felt lick my face…. The children saw me and they beckoned me to come over…. [W]hen I finally decided to step over…. then I felt this heavy tug, like a vacuum and then I was forced out and the next thing I knew I was back in my own body (Lindley, Bryan, and Conley 112).
Here another favorite insect of children is encountered in an NDE (cockroaches and mosquitoes are not reported) along with a very popular wild animal.
(10) In other NDEs sentient plants are encountered—one woman reported worrying about the flowers she was stepping on in her NDE, when the flowers telepathically communicated to her that they were alright! (Fenwick and Fenwick 86-87).
(11) Occasionally even dead celebrities are encountered in NDEs. In one of Moody’s cases a middle-aged woman from the Midwestern US who shook hands with Elvis Presley as a child reported encountering Elvis in her NDE. After having an OBE during surgery, she reported:
I then entered into a dark round tube or hole. I could call it a tunnel. I seemed to go headfirst through this thing and suddenly I was in a place filled up with love, and a beautiful bright white light….
As I walked through this meadow I saw people separated in little bunches. They waved to me, and came over and talked to me. One was my father who had died about two years before….
Just as I turned to go, as I felt myself being drawn back, I caught sight of Elvis. He was in this place of an intense bright light. He just came over to me, and took my hand, and said: ‘Hi Bev, do you remember me?’ (Morse and Perry, “Transformed” 109-110).
While an Elvis sighting in an NDE may not be as problematic for a survivalist interpretation as an encounter with a living person, it seems unlikely that a real glimpse of the afterlife would include a greeting from a deceased celebrity.
(12) In a case sent to Kenneth Ring from a Canadian researcher, another NDEr describes an exceptionally detailed NDE world where he encounters Albert Einstein. After touring spotless streets “that appeared to be paved in some kind of precious metal,” talking to a street sweeper, listening to a choir of angels, and viewing an art gallery:
Next we materialized in a computer room. It was a place of great activity, yet peace prevailed. None of the stress of business was present, but prodigious work was accomplished. The people seemed familiar to me, like old friends. This was confusing, because I knew there to be present those who lived on earth still, and those who had passed on. Some of them I knew by name, others by reputation; and all had time for me, to teach me if I ever need help understanding. One of them was Albert Einstein…. He asked me if I would care to operate the computer (Kellehear 14).
There is a fantastic quality to this story, such as transferring from place to place ‘instantly,’ as if by magic. The fact that this NDEr claims to see people who are still alive in this supposed afterlife environment also points to its hallucinatory nature.
(13) But if encounters with conscious plants, talking insects, and dead celebrities doesn’t give you pause about accepting NDEs as visions of an objective afterlife reality, perhaps NDEs that include encounters with fictional characters will. Morse reports that a 10-year-old boy had an NDE where he encountered a video-gaming wizard who loved Nintendo and said to him: “Struggle and you shall live” (Abanes 116). Karl Jansen similarly reports finding childhood NDEs that include encounters with video game and comic book characters:
Claims that near-death experiences are always identical, regardless of the set and setting, are contradicted by the variety actually found in published reports. They differ between people and cultures. For example, instead of a tunnel and angels, East Indians may describe the River Ganges and a particular guru. A child having a NDE may “see” his or her still-living friends and teachers, or Nintendo and comic book characters, rather than God (Jansen 96).
(14) In a collection of pediatric near-death experiences published in 1990, Serdahely even found a case where a girl encountered a favorite toy during her NDE—an old stuffed animal. Morse summarizes the case as follows:
A 10-year-old girl had a full cardiopulmonary arrest while in the intensive care unit after spinal surgery. She described her experience 2 years later. Stating she was “peaceful and relaxed, and remembered seeing a whitest blue light at the end of the tunnel. She saw the shadow of a dog, and also a white lamb that was loving and gentle, which led her back to her body.” Her parents reported at age 2, she had a lamb that doubled as a music box that was her favorite stuffed animal (Morse 62).
(15) One of the most bizarre types of NDEs are the ‘meaningless void’ experiences that often occur during childbirth. In a typical case, a 28-year-old woman became unconscious when given nitrous oxide during the birth of her second child, but when her blood pressure suddenly dropped, she reported:
I was aware … of moving rapidly upward into darkness. Although I don’t recall turning to look, I knew the hospital and the world were receding below me, very fast…. I was rocketing through space like an astronaut without a capsule, with immense speed and great distance.
A small group of circles appeared ahead of me, some tending toward the left. To the right was just a dark space. The circles were black and white, and made a clicking sound as they snapped black to white, white to black. They were jeering and tormenting—not evil, exactly, but more mocking and mechanistic. The message in their clicking was: Your life never existed. The world never existed. Your family never existed. You were allowed to imagine it. You were allowed to make it up. It was never there. There is nothing here. There was never anything there. That’s the joke—it was all a joke.
There was much laughter on their parts, malicious. I remember brilliant argumentation on my part, trying to prove that the world—and I—existed…. They just kept jeering.
“This is eternity,” they kept mocking. This is all there ever was, and all there ever will be, just this despair….
Time was forever, endless rather than all at once…. Yes, it was more than real: absolute reality. There’s a cosmic terror we have never addressed (Greyson and Bush 102).
Since meaningless void experiences paint a far-from-gleaming picture of what the dying sometimes experience, many New Age near-death researchers are reluctant to accept them as visions of another world. Ring, for example, ultimately concludes that meaningless void experiences “are not true NDEs as such but are essentially emergence reactions to inadequate anesthesia” (Ring, “Frightening” 20-21).
There is something disingenuous about Ring taking this position. On the one hand, Ring and like-minded researchers have argued that prototypical Western NDEs are evidence for an afterlife at least in part because they are consistent across accounts, feel real, and have a transformative effect. At the same time, Ring argues that meaningless void experiences are merely reactions to anesthetics, even though they are also consistent across accounts (different people report similar experiences), feel real, and have a transformative effect—albeit a negative one: “our preliminary observations indicate that ontological fear is a common result of the experience” (Greyson and Bush 109).
In fact, meaningless void experiences probably are reactions to anesthesia, given their rare incidence and tendency to occur during childbirth, when anesthetics are almost always administered. The point is that meaningless void experiences have the same characteristics that have been used to justify viewing more standard NDEs as glimpses of an afterlife, yet are rarely themselves seen as actual visions of another world.
Ring’s argument that meaningless void experiences are hallucinatory episodes triggered by anesthesia is significant. It is a tacit admission by a major near-death researcher that a person can have an experience near death that has commonalities with the others’ experiences near death, feels incredibly real, and produces lasting transformations, even though it is only a hallucination. If meaningless void experiences can be reasonably viewed as hallucinations, so can prototypical Western NDEs.
In her 1997 book In A World of Their Own: Experiencing Unconsciousness, Madelaine Lawrence has also acknowledged that persons sometimes experience hallucinations near death after finding reports of visions of the Grim Reaper in her cardiac patients.
(16) In 1926 Heinrich Klüver systematically studied the effects of mescaline (peyote) on the subjective experiences of its users. In addition to producing potent hallucinations characterized by bright, ‘highly saturated’ colors and vivid imagery, Klüver noticed that mescaline produced recurring geometric patterns in different users. He called these patterns ‘form constants‘ and categorized four types: lattices (including honeycombs, checkerboards, and triangles), cobwebs, tunnels, and spirals (Blackmore, “Dying” 68-70; Bressloff et al. 474).
Klüver’s form constants have appeared in other drug-induced and naturally occurring hallucinations, suggesting a similar physiological process underlying hallucinations with different triggers. But what is particularly interesting is that Klüver’s form constants also appear in near-death experiences.
After a heart attack, one man from the Evergreen Study had an NDE that included seeing a lattice (‘grid’) or cobweb, one of Klüver’s form constants:
The more I concentrated on this source of light the more I realized that it was a light of a very, very peculiar nature… it was more than light. It was a grid of power… if you could imagine the finest kind of gossamer spider web that was somehow all pervading, that went everywhere [ellipses original] (Lindley, Bryan, and Conley 111).
A similar NDE is reported in Johann Christophe Hampe’s early To Die is Gain, where NDE cases were compiled without knowledge of Moody’s Life After Life:
I was moving at high speed towards a net of great luminosity. The strands and knots where the luminous lines intersected were vibrating with tremendous cold energy. The grid appeared as a barrier that I did not want to move through, and for a brief moment my speed appeared to slow down. Then I was in the grid (Hampe 65).
Other form constants have also periodically appeared in NDEs. Zaleski notes that, among the variety of ‘paths’ that NDErs have taken to the NDE world, some NDErs have found themselves “spinning in vertiginous spirals” rather than traveling through a tunnel or darkness (Zaleski, “Otherworldly” 122). While tunnel experiences are well-represented in Western NDE reports, the occasional presence of other hallucinatory form constants in these reports (e.g., lattices, cobwebs, and spirals) suggests that NDEs are hallucinations.
Unfulfilled Predictions: Psychic Inability
Despite the contributions of serious neuroscientists, psychologists, sociologists, and anthropologists to the field, ‘near-death studies’ is rife with wildly irresponsible claims about NDErs gaining psychic abilities, healing powers, and accurate prophetic visions of the future after their NDEs. These unsubstantiated assertions recall those of crop circle researchers who have ‘discovered’ that the wheat found in crop circles has been genetically altered. Phyllis Atwater, for example, claims that NDErs look younger after NDEs when before and after pictures are compared and claims that NDErs’ ‘energy fields’ interfere with electronic devices like watches and microphones (though apparently not with the much more sensitive computers NDErs use).
Sadly, the most prominent representatives of the field—Raymond Moody, Kenneth Ring, Melvin Morse, Phyllis Atwater, and Margot Grey—have made all sorts of unsubstantiated and fanciful claims about NDErs’ paranormal abilities. While this alone seriously damages the credibility of their own work and mars near-death studies as a whole, the damage is exacerbated by wild New Age speculations on the meaning of the NDE from the very same researchers. Given such fringe claims, it should be no surprise that the mainstream medical community has viewed research into the near-death experience with suspicion.
In Heading Toward Omega, for instance, Ring claimed that many of his NDErs had ‘prophetic visions’ of the future of humanity, including earthquakes, volcanic eruptions, marked climate change, economic collapse, and humanity on the verge of nuclear annihilation. ‘Massive upheavals’ were to start in the 1980s and end with world peace just after the dawn of the new millennium (Fox 40-41).
But despite repeated assertions of widespread and even quite frequent paranormal abilities manifesting after NDEs (reported by NDErs themselves and endorsed by many near-death researchers), not a single experiencer, so far as I am aware, has ever volunteered for a controlled experiment to test their alleged psychic powers. Given that such a demonstration would easily validate their claims, one simple question begs for an answer: Why not?
Cases where NDErs’ predictions have failed to come to pass suggest that experiencers have not attempted to demonstrate their psychic powers experimentally because they have no powers to demonstrate. Apparently NDErs’ predictions are no different than those of other modern-day prophets—either vague enough to cover almost any event, or specific but unfulfilled.
(1) Dannion Brinkley’s self-reported psychic abilities after his NDE are an excellent example of unfulfilled predictions. After lightning struck the telephone line he was using in 1975, he was thrown across the room, laying on the floor looking up. His searing pain was replaced with a feeling of peace and he found himself looking down on his body until paramedics loaded him onto an ambulance. Next he reported seeing a tunnel forming in the ambulance which came to him and engulfed him while he heard rhythmic chiming. He noticed a light ahead and rapidly approached it until it surrounded him. A silver form emerged which he identifies as an empathetic ‘being of light’ emitting all the colors of a rainbow. The being engulfed him, causing him to review the events of his life. Next they both ‘flew’ into a city of crystalline cathedrals where Brinkley arrived at a ‘cathedral of knowledge.’ His guide disappeared, only to be replaced by 13 others behind a podium when he sat down on a bench. As each being approached him, a ‘box’ appeared on its chest which ‘zoomed’ out toward his face showing a ‘television picture’ of a future world event. Brinkley was restored to normal consciousness in the morgue just shy of half-an-hour since he was struck by lightning (Brinkley and Perry 4-31). He also claims to have gained spectacular psychic abilities since his NDE, but these have never been tested in any controlled experimental setting.
The prophetic visions shown to Brinkley during his NDE were often given dates in his best-selling Saved by the Light. They included visions of an Israeli settlement spreading into Jordan until Jordan was replaced by a new country (34). This was to be followed by a war between Israel and an alliance of Russia and a “Chinese-and-Arab consortium” over ‘some incident’ in Jerusalem (35). An alliance between Saudi Arabia, Syria, and China was to be made in 1992 to destroy the American economy, while Saudis were to give money to North Korea in order to destabilize Asian markets (35). By 1993 Iran and Iraq were predicted to have both chemical and nuclear weapons, including an Iranian submarine with nuclear missiles on a religious mission to stop the shipment of oil from the Middle East (41).
Brinkley claims to have foreseen the Chernobyl incident in 1986 and the 1991 Gulf War during his NDE, but these events occurred well before the publication of his book. Chernobyl was supposed to be followed by another nuclear accident in 1995 which contaminated a northern sea to the point that ships would not travel through it (36-37).
He also saw “border disputes and heavy fighting between Soviet and Chinese armies” over a railroad ultimately taken by the Chinese. The Chinese then invaded the Soviet Union and took over half of the USSR, including Siberian oil fields (39). Brinkley confesses that when he had these visions in 1975, he didn’t know that the Soviet Union would fall.
The collapse of the world economy “by the turn of the century” resulting in “feudalism and strife” was also predicted (39). The government closing of banks in the 1990s was to be followed by “the bankruptcy of America by the year 2000” (40). America would cease to be a superpower “sometime before the end of the century” due to two horrific earthquakes, perhaps near some body of water. Rebuilding after the quakes was to weaken the economy to the point that starving Americans waited in long lines for food, again, before 2000 (40).
Brinkley envisioned a terrorist attack on France prior to 2000 where a chemical was to be released into a French city’s water supply, killing thousands, in response to the French publication of “a book that infuriates the Arab world” (41).
Brinkley also saw the collapse of democracy and its replacement with a fundamentalist government in Egypt in 1997 (41). In his final visions he saw people in towns all over the world eating their dead out of desperation, “weeping as they cooked human meat” (42). Meanwhile, wars in Central America and South America broke out, leading to the formation of socialist governments in all of the countries of this region before 2000. As a result, millions of refugees crossed the American border, forcing the US government to deploy troops to the border to push the refugees back across the Rio Grande, destroying the economy of Mexico (45). Again, all of this (and more) was predicted to happen before 2000.
Elaborate as these visions are, none of the events predicted to occur after Saved by the Light was published in 1994 have come to pass. The prophetic visions Brinkley gained during his NDE appear to be no different than those of any other run-of-the-mill prophet. Even the Fenwicks comment that while “pre-publication happenings came into Dannion’s head with pinpoint accuracy,” “those events due to take place after 1994 are foretold with less precision” (Fenwick and Fenwick 167). Brinkley did tend to be vague in places—omitting dates or using phrases like “some incident” or “sometime before the end of the century.” But his predictions were precise enough for us to recognize not only that they never came to pass when he predicted they would, but that nothing even close to those events came to pass.
It would not be surprising for NDErs to come back from ‘the other side’ with vague or false predictions if near-death experiences are really a particular kind of brain-generated hallucination. But if NDEs were literally journeys of one’s soul or double into ‘the next world,’ it would be surprising for denizens of that realm to offer false information. In Brinkley’s case particularly, it would be surprising for otherworldly beings to provide him with accurate predictions about future events occurring before the publication of his book, but false predictions about future events occurring after the book is published. Dare I suggest that Brinkley just might have exaggerated claims about the accuracy of his pre-publication predictions?
(2) Exaggerated claims of psychic power are not limited to NDErs who write best-selling books about their experiences. In an interview with a woman who had three NDEs, journalist Art Levine sought to test her reputed psychic powers. Among other things, the woman claimed to have predicted the terrorist attacks on the World Trade Center and Pentagon on September 11, 2001. Levine notes that, although he carelessly supplied some information about his life to the woman, she revealed nothing about him that couldn’t have been guessed by the average person and many of the details she provided were flat wrong:
[G]ood psychic readings—though still unproven by the hard tests of science—should have more hits than misses, without any cue from the client….
Her initial results were promising. During that first interview, for instance, she casually demonstrated her skills by asking, “How’s your low-back pain doing?” and mentioning in a vague way problems I’d had with my father. I didn’t know whether to be amazed or just chalk it up to a lucky guess anybody could make about a middle-aged Jewish guy….
After a long wait, she began speaking. “You had two avenues of education, but you took a break in one and totally shifted gears,” she pronounced. Since I always intended in college to be a writer, even though I dropped a course or two along the way, Shoemaker’s reading wasn’t off to a very promising start. Later, when discussing my work, she claimed that I once planned to have a medical career, but now, as an investigative reporter, “you’ve gone into medicine through the back door.” Wrong again: I never once in my life thought of becoming a health professional….
I became worried when she claimed that I was developing Crohn’s disease, a serious, painful inflammation of the small intestine. But because she also asserted that I suffered from regular headaches, I felt relieved—that’s one health complaint I don’t have. But since I’m actually at risk of digestive problems because of an anti-inflammatory medication I take, I didn’t take chances: I later asked my doctor to look for signs of the dreaded Crohn’s disease. There weren’t any.
She didn’t seem to be much more accurate when discussing my parents. “I get a missing of the father. It’s almost like he’s not around; you’re not able to converse as much. The brilliance of his mind isn’t the same,” she said. Later, she gave additional poignant insights: “Your father’s health is wavering.” There is, as it turns out, a good reason for all this: He’s dead, a little detail that she missed. She also described my mother: “I get your mother as spunky. She can be quite feisty, and she has her own set of rules.” Perhaps, in the afterlife, she has adopted this new personality. She died several years ago in a tragic accident, but when she was alive, she was generally bossed around by my domineering father (Levine).
These cases demonstrate that some NDErs are given false visions of the future in their NDEs or get a false sense of having psychic powers they do not have. Of course this isn’t flatly inconsistent with a survivalist interpretation of the NDE; perhaps otherworldly beings supply us with false information during NDEs or NDErs become more skilled at self-deception than ESP after their experiences. But false prophecy and psychic inability are exactly what we would expect to obtain if NDEs were not really journeys into another realm. Moreover, the proclivity of many NDErs to claim paranormal abilities they do not have should make us suspicious of uncorroborated claims of veridical paranormal perception during out-of-body experiences in NDEs.
Conclusion
Many near-death researchers clearly interpret NDEs as evidence for survival of bodily death. Because many people would like to know that there is an afterlife rather than simply take the notion on faith, it not surprising that the study of NDEs tends to attract researchers who already believe that NDEs provide evidence for survival. NDEs seem to be a natural lure to survivalists, since they offer the prospect, at least, of bolstering such researchers’ belief in survival after death and of offering them hints about what exactly is going to happen to them when they die. Thus it is hardly a revelation that many of the researchers investigating the phenomenon are confident that NDEs point toward the reality of survival of bodily death.
But how do near-death researchers obviously sympathetic to the survival hypothesis explain hallucinatory NDE characteristics? Typically, they invoke a rather ad hoc rationalization: whenever culturally conditioned or other clearly hallucinatory features are found, the NDEr must have made a mistake. For example, one could argue that when NDErs report encountering living persons ‘on the other side,’ they must be misidentifying the person seen. When a Christian sees Jesus in an NDE while a Hindu sees Yamaraj, the standard explanation near-death researchers give is that both are seeing the same spiritual being but ‘interpreting’ it as a specific religious figure. But how do we know that the Christian didn’t really encounter a being that looks exactly like portraits of Jesus, or that the Hindu didn’t encounter a being with the specific features his culture ascribes to Yamaraj?
Aside from cases where the persons encountered during NDEs are obviously culture-bound projections or could not possibly reside in the afterlife at the time of the experience, many near-death researchers urge us to take what NDErs report at face value. If an NDEr reports feelings of peace, an OBE, traversing a tunnel, and entering an illuminated garden where he encounters his deceased grandfather, researchers often advocate interpreting the account literally as a vision of the afterlife. We are typically encouraged to think that the NDEr really left his physical body, traveled through the physical world in a disembodied or astrally embodied state, traversed a tunnel from the physical world to a transcendental realm, and actually communicated with his deceased grandfather. It is only when an NDE contains obviously hallucinatory features that such near-death researchers resist interpreting it as a literal glimpse of the afterlife.
Here survival proponents urge us not to take NDErs’ accounts at face value; at the same time, they expect us to accept the ‘core NDE’ as reflecting some afterlife reality. The standard explanation of NDE features inconsistent with literal glimpses of an afterlife are interpretative embellishments, but that the core NDE—whatever that is said to be—really reflects another reality which awaits us after death. Morse, for example, writes: “The core NDE is then secondarily interpreted according to the age and culture of the person experiencing the event” (Morse 70). Atwater, by contrast, implies that living persons seen in NDEs either represent an early hallucinatory phase of an otherwise veridical experience or are comforting disguises taken on by transcendental beings:
There is another greeter, though, who is sometimes encountered—a living person—more commonly reported by children than by adults. This may be a favorite teacher, the kid down the block, a friend or a relative. Does this fact call into question the validity of near-death imagery? No, and here’s why.
In every case I have thus far investigated where this occurred, the living greeter did not remain in the scenario any longer than it took to alert or relax the experiencer. Once that happened, the living greeter disappeared, and imagery more common to near-death states emerged as the episode deepened. It is almost as if the sole purpose of living greeters is to ensure the continuance of the episode so that it can become more meaningful. They don’t “stick around” like other greeters usually do (Atwater 12).
No doubt recalcitrant proponents will simply continue to give a new spin to evidence that otherwise appears to falsify a survivalist interpretation of NDEs.[32]
While some near-death researchers weave elaborate schemes to explain away inconsistent evidence, others deride those who disagree with their questionable conclusions by impugning their motivations. For instance, Charles Tart, a parapsychologist well-known for conducting OBE experiments, implicitly accuses all researchers who view NDEs as hallucinations of ‘scientism.’ ‘Scientism’ usually refers to a dogmatic adherence to the prejudices, paradigms, or presuppositions ‘fashionable’ among contemporary scientists. Such an accusation is intended to convey the idea that mainstream scientists have been ‘blinded’ by their prejudices from acknowledging the ‘obvious’ evidence that we do in fact continue on after death.
Scientism is an epithet typically hurled at anyone who defends a mainstream scientific position against the views of an unconventional minority. But Tart gives scientism a more specific definition: “a dogmatic commitment to a materialist philosophy that ‘explains away’ the spiritual rather than actually examining it carefully and trying to understand it” (Tart 74). Right off the bat, it is evident that Tart presumes (1) that materialism is false, (2) that a spiritual realm actually exists (if our goal is “trying to understand it” we must presume it exists), (3) that there are ‘spiritual data’ which cannot adequately be explained by materialism and (4) that anyone who rejects the existence of a spiritual reality has failed to carefully examine the evidence.
As will become clear shortly, the only purpose of an appellation of scientism in Tart’s discussion is to persuade an audience to dismiss the views of researchers who view NDEs as hallucinations on the grounds that they are biased by prior beliefs (as if Tart doesn’t have any prior beliefs that incline him toward a survivalist interpretation of NDEs). But this is just a distraction from the real issue; the real issue is whether or not OBEs and NDEs provide unambiguous evidence for survival of bodily death. If they did, Tart would not have to resort to accusations of bias; he could simply document the evidence showing that survival of bodily death occurs, just as biologists can document the evidence showing that species evolve over time. But, in fact, the issue remains a contentious one, even among parapsychologists. As Carlos Alvarado, a former president of the Parapsychological Association, concedes:
The dominant model in OBE studies, by far, is the psychological one…. There are many reasons for the domination of this model. One is the fact that contemporary psychology, as well as science at large, is hesitant to propose explanations that contradict current paradigms. But in all fairness, it should be noted that little evidence exists to support the projection model [i.e., that something leaves the body during an OBE]; furthermore, this model presents myriad obstacles to scientific testing (Alvarado 201).
Indeed, most parapsychologists today are not convinced by the available evidence that survival of bodily death is likely to occur, even if they would like to believe that it will. For example, John Beloff, a parapsychologist who certainly cannot be accused of scientism and who has no sympathy at all for materialism, writes specifically of NDEs that:
[The near-death experience] remains open to a wide variety of psychological and physiological explanations—such as cerebral anoxia, or oxygen starvation of the brain, a self-defensive strategy in the face of imminent extinction, and so forth. At all events, it would be premature to interpret it at face value as affording a vision of the next world [emphasis mine] (Beloff 267).
The rhetoric pervading Tart’s account implies that scientism or dogmatic materialism is the only obstacle to accepting a survivalist interpretation of NDEs. But this is simply not the case. First, it is crucially important to note that one could have good reasons for disbelieving that NDEs are visions of an afterlife without accepting materialism. For instance, this essay has actually presented data which suggests that NDEs are not glimpses of another world after death. One need not have any commitment to materialism—dogmatic or otherwise—to doubt that genuine glimpses of an afterlife would involve train rides, false out-of-body perceptions, or encounters with living persons, fictional characters, and mythological creatures. It is entirely possible that an afterlife exists but that NDEs are not glimpses of it—a view similar to the Buddhist belief that the dying pass through several illusory bardo states generated by their own minds before entering the ‘real’ afterlife (Fox 94-96).
Second, there may be good independent grounds for holding materialism to be true, such as the massive amount of evidence for the dependence of consciousness on the brain. A commitment to materialism, then, need not be based on “an emotional attachment to a totally materialistic view of the world” (Tart 75). One may come to believe that materialism is probably true—as many contemporary scientists and philosophers have—simply because physicalistic explanations of uncontroversial phenomena have been so successful. The conclusion that materialism is probably true may simply be an eminently reasonable inference to the best explanation.
Further along in his discussion, Tart’s rhetoric becomes even more blatant. In his discussion of scientism, he implies that anyone who denies that NDEs provide evidence for survival or rejects the reality of survival after death altogether must be blinded by scientism[33]:
They don’t recognize that their belief that everything can be explained in purely material terms should be treated like any scientific theory, i.e., it should be subject to continual test and modified or rejected when found wanting (75).
As already noted, though, one can believe that NDEs are not good evidence for survival or even that survival after death never happens without believing that “everything can be explained in purely material terms.” David Chalmers, for instance, has recently defended a version of property dualism (in The Conscious Mind) that denies that the mind can be explained in purely physical terms while also denying that the mind can exist independently of the brain (or some physical substrate); but the latter is a prerequisite for the sort of life after death Tart envisions.
Moreover, even those who believe that “everything can be explained in purely material terms” might acknowledge that this belief is just a hypothesis capable of being falsified. That is, one can accept materialism while simultaneously acknowledging that some evidence—if present—would refute it. The issue for these open-minded materialists, then, is not whether any evidence could refute materialism, but whether the sort of evidence that could refute it has actually been produced. And most materialists, I suspect, would deny that such evidence actually exists, even though they could imagine what sorts of evidence would falsify materialism.[34]
By implying that those who reject NDEs as evidence for survival are advocates of some pernicious scientism, Tart presumes that the very issue of contention has already been resolved: that NDEs really are evidence for survival of bodily death. But, of course, this conclusion has not been established beyond a reasonable doubt; in fact, it is not even clear that the survivalist interpretation of NDEs is more likely to be true than false. Moreover, Tart fails to recognize that there are perfectly legitimate reasons for maintaining that NDEs are not visions of an afterlife—reasons that I have outlined in this essay because few people who’ve thought about NDEs have even been aware of them.
Endnotes
[1] A slightly different version of this paper was published in three parts in three consecutive issues of the Journal of Near-Death Studies in 2007, but this online version has been updated to reflect the final content of those three lead papers, as well as some material which I cut from those issues for space. Each part was followed by three or four commentaries and my reply to the commentaries. In her commentary on this part of this paper, Janice Holden conceded that this World War II case was a plausible candidate for a hallucinatory NDE. However, she rightly noted that it is open to an equally plausible alternative explanation:
[W]e cannot know how much time passed or what transpired in the material world while the NDEr’s consciousness was purportedly elsewhere. We know only that when the NDEr perceived his consciousness to have returned to his body, “the Heinkels were still firing.” That firing may have been a subsequent strike following the initial one in which the NDEr’s body rose and fell; hence, the cook’s demise may have occurred not during the initial but during a subsequent strike, after the NDEr had “left” the material world (Holden, “Heaven” 35-36)
Holden added that this would not only explain the NDEr’s failure to see what remained of Osman the cook, but the Bren gunner’s disappearance as well, for the Bren gunner “might have left in the interim” (36).
[2] Janice Holden suggested that Mrs. Davey’s failure to see her body while ostensibly ‘up on the ceiling’ may have merely been an instance of “incomplete visual perception” rather than hallucination (Holden, “Heaven” 37). However, she notably cited Margot Grey’s discovery that some out-of-body NDErs could not see their physical bodies even when they explicitly wanted to see them (which is difficult to reconcile with the assumption that OBEs involve genuine perception of the physical area where the body would be), and in my reply I noted that in the majority of Oliver Fox’s induced OBEs, Fox reported being unable to find his physical body lying on the bed despite explicitly looking for it there. I also noted that out-of-body discrepancies involving clearly false perceptions—such as Robert Crookall’s report of an OBEr who saw bars on his bedroom window that didn’t exist—cannot be explained by selective attention to detail or preoccupation with something other than the location of one’s physical body.
[3] In his commentary Peter Fenwick noted that spontaneous OBEs, OBEs accompanying sleep paralysis, REM sleep OBEs, electrically stimulated OBEs, OBEs accompanying epileptic seizures, and cardiac arrest OBEs all arise from different physiological mechanisms. Of these subtypes, Fenwick stated that he finds OBEs occurring during cardiac arrest to be the most interesting because of the possibility that they occur when the brain has reached “electrical silence” (Fenwick 47).
Fenwick seems to be driving at two different points here. First, he seems to be arguing that is unlikely that different physiological mechanisms would produce the same illusion of perceiving outside of the body, but that it would not be surprising for there to be different physiological triggers of an experience that actually occurs outside of the brain. But as Harvey Irwin has pointed out, the crucial physiological state common to most kinds of OBEs may be extremes of cortical arousal, from the very low arousal accompanying meditation or induced OBEs, to the very high arousal accompanying a near-death crisis, coupled with psychological traits such as a high capacity for absorption and a strong need for absorbing experiences (Irwin, “Flight” 303; Irwin, “Domain” 6).
Second, Fenwick seems to be conceding that most OBEs may very well be hallucinatory (as he notes that most spontaneous OBEs that are not near death “are probably dissociative states in which the experiencer will gain no veridical perception away from the body”) (Fenwick 46), but that cardiac arrest OBEs might very well involve genuine perception outside of the body (since he writes that it is “important to test and to verify objectively whether the experiencer really did have the NDE when unconscious and was able to gain veridical information”) (47). But it is notable that several of the clearly hallucinatory NDEs I cite here accompanied events surrounding cardiac arrest, such as when one NDEr perceived himself flying backward in time with a formation of swans, another NDEr reported being interrogated by nurses about subversive activities, and yet another NDEr felt he was about to be devoured by giant fangs.
[4] Predictably, Janice Holden objected that the mere fact that some NDEs may be hallucinations does not logically entail that all NDEs are hallucinatory (Holden, “Heaven” 38). While this is undoubtedly true, the existence of hallucinatory NDEs does give us some grounds to doubt that any NDEs are experiences of a transcendental realm. Consider an analogy: Suppose that there is some subset of “alien abductees,” typical of other alien abductees in almost every respect, except that these abductees report abductions that allegedly occurred in very public places. Suppose further that others present at these places at the time of the alleged incidents deny witnessing any extraterrestrial kidnappings, despite having been in a position to observe such incidents had they occurred. Setting aside ad hoc explanations for such discrepancies, such as that extraterrestrials must have erased the memories of those present, it is certainly reasonable to conclude that these alien abductees’ reports were derived from their imaginations. Wouldn’t the discovery of discrepant experiences, similar in all other respects to other alien abduction experiences, also make it reasonable to doubt that any alien abduction experiences were caused by actual extraterrestrial visitation—especially when there has never been even one indisputable case of extraterrestrial visitation?
William Serdahely similarly suggested that, because they are uncommon, hallucinatory NDEs are not problematic for a survivalist interpretation of NDEs (Serdahely, “Commentary” 52). But this does not follow. As I pointed out in my reply, only a small fraction of memories of Satanic ritual abuse, for example, might be demonstrably false, as only a small fraction of them include details that can be checked later, such as memories of the disposal of human remains. Reports of discrepant NDEs are always going to be at least as infrequent as NDE reports that include details which can be checked against reality later, and most NDE reports lack such details.
[5] In his first commentary Bruce Greyson denied that near-death researchers ever appeal to such “‘high probability’ guesses” when making a case for veridical paranormal perception during NDEs—which is a bit too strong given that such instances can be cited. (In fact, in my response I cited three examples of ‘high probability guesses’ proffered by near-death researchers). More importantly, though, Greyson maintained that there have been cases of NDErs accurately reporting quite unpredictable details, noting for instance “one man’s accurate description of his cardiac surgeon during his open-heart surgery ‘flapping his arms as if trying to fly’,” a detail which Greyson described as “corroborated by independent interviews with the doctors and nurses involved” (Greyson, “Paranormal” 240). (The surgeon in question had developed a habit of keeping his arms close to his chest and pointing with his elbows to keep his hands sterile.)
But psychologist David Lester had already noted that the ‘corroboration’ for this case was sorely lacking, writing in an earlier book:
The case [Emily Williams] Cook [and coauthors Bruce Greyson and Ian Stevenson] felt was most supportive [of veridical paranormal perception during NDEs] was that of a 56-year-old man who was operated on for quadruple bypass surgery. During the surgery, he had a near-death experience, including the sensation of floating out of his body and observing the operation. In particular, he described the surgeons working on his leg (they stripped some veins to create a bypass graft) and one of the team flapping his arms as if trying to fly, a gesture which that surgeon habitually made during surgery. The patient wrote the experience down in 1990, and Cook’s team interviewed the surgeons in 1997. The surgeon who flapped his arms did not recall whether he did so or not, and the other surgeon did not recall him doing so, although he did confirm that the patient reported the experience immediately after the surgery.
In this case, the best case that Cook could produce, the experience was not recorded for two years and the surgeons were not interviewed until nine years had passed. Given that many patients report near-death experiences and that many of the researchers (such as Ian Stevenson and his team) are located in a university with a medical school, it is amazing that no case has yet appeared in which a near-death experience (let alone one with the features that Cook focused on) has been recorded (with audio or video recorders) immediately after the patient recovered and the details checked there and then. This needs to be done, and it is surprising that it has not yet been done [emphasis mine] (Lester 96).
[6] In his commentary William Serdahely pointed out that standard hallucinations do not produce the largely positive transformations that typically follow NDEs (Serdahely, “Commentary” 52-53). This is indeed an important difference that requires an explanation, but as I pointed out in my reply, one is not hard to fathom. First, there is no doubt that some (but importantly not all) of the transformation experienced by NDErs is due simply to having been close to death; but past proximity to death (and the reevaluation of one’s life that presumably follows it) provides a significantly different context for NDErs compared to hallucinators in general. Second, I hypothesized that the more robust transformations found among NDErs, compared to those who came close to death without experiencing an NDE (Bonenfant 155; Groth-Marnat and Summers 110; van Lommel et al. 2043), are a result of the tendency of Western NDErs to give their NDEs a survivalist interpretation. A prospective study asking NDErs how they interpret their experiences, clearly dividing them up into survivalist, nonsurvivalist, and uncertain interpreters, would provide a direct test. If my hypothesis is correct, nonsurvivalist NDErs should have transformations comparable to those found among non-NDErs who came close to death.
[7] Cognitive psychologist Jason Braithwaite points out that the Fenwicks put themselves in a bind by making this argument, for if the brain is so impaired during an NDE that it is incapable of generating a coherent experience, then it is also too impaired to encode a memory of any experience occurring during that time, even if that experience occurred ‘outside’ of the brain. So the fact that NDEs are remembered implies that they occur when the brain is still functioning well enough to encode memories, and thus also functioning well enough to generate experiences (Braithwaite 12).
[8] Although this prospective study relied on NDErs’ self-reports of transformations following NDEs, previous and subsequent retrospective studies have sought and found corroboration from others of the reality of these transformations. They are not simple artifacts of biased self-assessment (Bonenfant 155; Groth-Marnat and Summers 110).
[9] The findings of the life-change inventory questionnaire at 2-year and 8-year follow-ups for NDErs and non-NDErs who come close to death are nicely summarized in Table 5 (van Lommel et al. 2042). From this table it is obvious that there are significant changes in social, religious, death, and other attitudes in NDErs between the 2-year and 8-year follow-ups. A similar pattern applies to non-NDErs, but NDErs reported higher initial scores (at the 2-year follow-up) than non-NDErs for the 13 categories listed. Generally, non-NDErs who came close to death did not believe in life after death at the 2-year follow-up and this belief had not changed at the 8-year follow-up. Non-NDErs’ interest in spirituality had also significantly decreased between the 2-year and 8-year follow-ups. By contrast, belief in life after death had increased slightly while interest in spirituality had markedly increased in NDErs between the 2-year and 8-year follow-ups. NDErs’ social attitudes and interest in the meaning of life had also markedly increased between the 2 and 8-year follow-ups.
[10] In his first commentary Bruce Greyson noted that he had just published a more definitive study on the possible role of embellishment in NDE reports. In his follow-up study 72 NDErs who had completed the Greyson NDE Scale about two decades earlier were asked to fill it out again without reference to their earlier scores (Greyson, “Consistency” 407). Because no statistically significant differences in the two sets of results suggesting embellishment were found, Greyson concluded that these NDE accounts were not embellished within the two-decade period between the two different administrations of the scale.
I should note that Greyson and I agree that had any embellishment occurred within the on average 17.7 years between the NDE and the first administration of the Greyson NDE Scale, this study would not have found it, for it was not designed to look for it. However, it is important to note that even within the period between the two administrations of the scale, the follow-up study fails to rule out the possibility of subtle embellishment of the sort that would not be measured by the Greyson NDE Scale. In my reply to Charles Tart’s commentary, for example, I asked whether a hypothetical change in how Pam Reynolds described her hair (namely, how it was shaved) would have even been detected by such limited measurements of embellishment.
In the case of the Greyson NDE Scale, evidently any such change would go undetected: the only relevant question to that detail would be whether she had seemed “to be aware of things going on elsewhere, as if by extrasensory perception,” a question that she would’ve answered “Yes, and the facts have been checked out” on both hypothetical administrations even if a description of her hair had changed. Simply put, Greyson’s follow-up study would not be able to detect if an NDEr recounted additional “veridical details” or “prophetic” visions than those that were first reported. It would only be able to determine if later reports included such elements when they were entirely absent from the initial reports—a gross rather than subtle change. Although I made my point slightly clearer when responding to Tart, I regret failing to fully spell it out (as I do here) when directly responding to either Greyson or Tart’s commentary, as my lack of specificity evidently led to a misunderstanding about exactly what I was arguing. In a letter to the editor in the next issue (to which I did not respond), Greyson pointed out that his finding applied to the “paranormal” features measured by the scale as much as it did to the overall scale scores. But my concern was with potential changes in NDE accounts that, if they existed, would not produce changes in either overall scale scores, or changes to answers to specific subsets of scale questions. Since the scale questions are rather general, my concern was with the possibility that changes in NDE accounts might occur that the scale simply would not measure.
[11] In a recent assessment of “the factual and logical errors present in the analysis proposed in the van Lommel et al. study” (Braithwaite 8), Jason Braithwaite independently raises similar objections to the typically overreaching conclusions of near-death researchers. For example, he notes the tendency of those with survivalist inclinations to mischaracterize what the dying brain hypothesis actually says about the role of anoxia in NDEs, only to force the conclusion that the hypothesis cannot account for the data on actual anoxic conditions during cardiac arrest.
He notes, for instance, that dying brain proponents have insisted all along that “it is the rate of change or rate of anoxia onset that is important, not the overall level reached” (10), such that the oversimplification of the dying brain hypothesis presented by van Lommel et al. amounts to a straw man. If that wasn’t bad enough, the authors attempted to refute their caricature with supposition rather than actual data. In place of actual measurements of cerebral blood gases, they appealed to dubious guesswork: “The presence and level of anoxia was indirectly inferred via experiential components provided in questionnaire responses and medical information regarding the nature and duration of the cardiac arrest” (9). So their entire argument, even setting aside its dubious details, is based on the mere assumption “that patients had comparable levels of anoxia” (9). Worse still, we already know that the subjects of G-LOC experiments do have comparable rates of anoxia since “the amount of G-force can be controlled, yet clear differences across individuals exist…. So a given level of anoxia can impact on experience differently across individuals” [emphasis mine] (10).
As Braithwaite notes at the outset, the data obtained from the landmark van Lommel et al. study are invaluable, but the conclusions of its authors do not follow from that data (8). His summary conclusion is apt: “[T]he paranormal survivalist position … sets out assuming the truth of that which it seeks to establish, makes additional and unnecessary assumptions, misrepresents the current state of knowledge from mainstream science, and appears less than comprehensive in its analysis of the available facts” (14).
[12] Jason Braithwaite similarly points out that the van Lommel et al. data causes a conundrum for a survivalist interpretation of NDEs: “[I]f the afterlife existed in some real sense, the real question is why did only 18% glimpse it?” (Braithwaite 10). Survivalist responses to this question are not hard to anticipate; however, what matters is not whether there are conceivable answers, but whether there are adequate ones.
For example, consider the simple survivalist response that perhaps every person who comes as close to death as possible without actually dying does encounter an afterlife, but (for whatever reason) rarely remembers their encounters. This is a conceivable answer, but one that is offered at a great price. For unless there is some independent reason to believe that ostensible non-NDErs who came close to death actually did have NDEs, but simply have no memory of their experiences, invoking total amnesia amounts to an unfalsifiable and entirely ad hoc attempt to save a survivalist interpretation in spite of contrary evidence. In other words, if one is going to be intellectually honest, the paucity of reported NDEs among those who come close to death strongly counts against the notion that NDEs are visions of an afterlife. For prior to actually reviewing the data, one would expect reports of such visions to be pretty pervasive among those who came close to death if NDEs were truly visions of an afterlife. Invoking the ad hoc hypothesis of amnesic NDEs—a hypothesis for which we have no independent evidence—allows one to keep a survivalist interpretation of NDEs on the table, but at the cost of contorting that interpretation to explain away any data that might count against it. It amounts to an ideological attempt to fit the data to one’s theories, rather than a scientific attempt to fit one’s theories to the data.
[13] Under the auspices of the Human Consciousness Project, Sam Parnia not only unveiled the AWARE and BRAIN-1 studies in a presentation to the United Nations, but also (52m:45s into the streaming archive) alluded to the forthcoming launch of a third study in the cardiothoracic unit of the University of Montreal designed to find out whether NDEs ever occur during deep hypothermia (rather than before or after it), a time when the brain cannot possibly be generating conscious experiences. Like AWARE, this third study will presumably also involve NDE target identification experiments, as veridical perceptions (or bodily sensations) during NDEs provide the only means by which researchers could correlate the timing of an NDE to a specific period of time during general anesthesia. Survivalists undoubtedly hope to correlate veridical paranormal perceptions during NDEs to a period of complete brain inactivity accompanying deep hypothermia.
[14] In a promotional interview for his book The Scalpel and the Soul, neurosurgeon Allan Hamilton claims to have witnessed a case of veridical perception during deep hypothermia (and thus during the complete cessation of electrical activity in the brain) reported by a certain ‘Sarah Gideon.’ In the book we are told that Gideon accurately recounted a number of details about operating room conversations that only could have occurred during her 17-minute period of brainstem inactivity, such as a nurse’s description of her engagement ring and where it was purchased, where and how her fiancé proposed to get married, and so on. Unfortunately, as is so often the case with such sensational accounts, the entire case appears to be a literary invention. As noted on the news page of the North-California IANDS Chapters website, in response to follow-up inquiries from Michael Tymn and Titus Rivas, Hamilton revealed that this remarkable case was an “amalgam” of different NDE accounts (one of which evidently was the celebrated Pam Reynolds case) meant only to be “illustrative.”
This report is reminiscent of Larry Dossey’s account of a certain ‘Sarah’ who reputedly made numerous veridical observations during a near-death OBE despite having been blind since birth. In response to an inquiry by Susan Blackmore about the whereabouts of this remarkable woman, Dossey similarly revealed having invented her:
‘Sarah’s’ story was a composite—the only composite story in the entire book, Recovering the Soul. My key reasons for composing her were to dramatically illustrate the key features of non-local ways of knowing—ways that seem (to me) fully documented in the experiences of diverse numbers of human beings. The ‘fact’ that Sarah was congenitally blind was a way of illustrating that non-local ways of gaining information bypass the senses and are ultimately independent of the brain (Blackmore, “Dying” 131-132)
[15] It is notable that philosopher of science Neal Grossman, who blithely dismissed the arguments and evidence offered in the print versions of this paper as “mere ideology” (Grossman, “Debunkers” 238), is one of the commentators who has most egregiously misrepresented and overstated the significance of the Pam Reynolds case, writing:
Perhaps the “smoking gun” case is the one recently described by Michael Sabom (1998). In this case, the patient had her NDE while her body temperature was lowered to 60 degrees, and all the blood was drained from her brain: “her electroencephalogram was silent, her brain-stem response was absent, and no blood flowed through her brain” (Sabom 1998, p. 49). A brain in this state cannot create any kind of experience. Yet the patient experienced a profound NDE, which included detailed veridical perception of the operation. Those materialists who believe that consciousness is secreted by the brain, or that the brain is necessary for conscious experience to exist, cannot possibly explain, in their own terms, cases such as this. An impartial observer would have to conclude that not all experience is produced by the brain and that, therefore, the falsity of materialism has been empirically demonstrated. Thus, what needs to be explained is the abysmal failure of the academic establishment to examine this evidence and to embrace the conclusion: materialism is false, and consciousness can and does exist independently of the body (Grossman, “Afraid” 7).
I’ll leave it to the impartial observers who have read the Pam Reynolds section of this paper, and who may not be nearly so eager to overthrow materialism at all costs, to draw their own conclusions.
[16] It is also notable in this regard that, in general, claims that NDErs had their experiences during a period of flat EEG are highly dubious for a variety of reasons. First, patients’ EEGs are rarely being recorded when a near-death episode occurs. Second, even in those rare cases where there actually are accompanying EEG recordings during such a crisis, in the chaos of an emergency, technicians are particularly likely to set up an EEG machine incorrectly, thereby producing inaccurate tracings (Moody 102). Cognitive psychologist Jason Braithwaite provides a simple example: NDE studies “making large claims about flat EEGs provide no information regarding the level of gain employed on the EEG device…. [even though] any EEG can become almost flat with the gain turned to a minimum. A flat EEG at maximum gain would be more indicative of neocortical inactivity, though again, not full-brain inactivity” (Braithwaite 11). On that note, third, standard EEG monitors only measure surface brain activity, failing to register the activity of deep brain structures like the brainstem (Braithwaite 11; French 362). Ali Henri Bardy notes that because normal EEG techniques “can detect electrical activity in only one half of the area of cerebral cortex” while “activity in the other half and deeper structures cannot be observed” (Bardy 2116), clear consciousness has yet to be shown “to occur in people without cerebral blood flow” (2116). And as Braithwaite points out, even localized cortical activity is sometimes undetectable in EEG readings. One study comparing functional magnetic resonance imaging (fMRI) data against patients’ corresponding EEG data during seizures
found significant increases in localised cortical neural activity (indicative of a seizure) in the fMRI BOLD (blood-oxygen-level dependant) response, which was completely absent from the EEG data…. despite the fact that the intense seizure activity occurred in a region where EEG electrodes were closely spaced…. [T]his is striking as the EEG completely missed the most intensely discharging region despite the fact that this region was also located at the cortical level (Braithwaite 11).
Finally, as in the Pam Reynolds case, even when more comprehensive EEG monitors are used in a controlled setting where a near-death episode is intentionally induced, there is no reason to believe that any resulting NDEs occurred during such periods, rather than before or after them (Woerlee, “Cardiac” 239-241).
[17] On this point, Michael Sabom responded: “The question here is not when Reynolds’s NDE began, but when it ended. Reynolds described her NDE as an uninterrupted, continuous experience” (Sabom, “Commentary” 258). Similarly, in his immediately preceding commentary, Charles Tart wrote that although Pam’s veridical perceptions occurred well before standstill, her description “implied quite clearly that her NDE went on all through the standstill, to and beyond the reinfusion of warmed blood” (Tart, “Commentary” 252). He consequently argued that denying Pam’s timeframe “ignores experiential evidence” (253).
However, as I pointed out in my response, without any verifiable perceptions from which to timestamp aspects of her NDE, Pam had no more means than anyone else to correlate specific parts of her subjective experience to specific events in the operating room. This simple point of logic is undeniable; there simply is no relevant experiential evidence aside from the independently verifiable aspects of her account and the sequence of events she reported.
Moreover, contra Sabom, when Pam’s NDE began is surely relevant to assessing the plausibility of when it ended. When it began is also a rather significant point when one considers that, had hypothermic cardiac arrest been postponed for another day sometime after she had already been anesthetized for an hour and a half, she evidently would have had her NDE without ever even approaching clinical death during the procedure. And although the large block of time between her veridical perceptions and the induction of hypothermia makes it quite plausible that her entire NDE occurred before her blood was cooled, it is still possible that her experience started before hypothermia was induced, ended when she sank into unconsciousness as hypothermia deepened, and resumed with the restoration of brain activity accompanying the reinfusion of warm blood.
Against this latter possibility, Sabom wrote that Pam’s NDE felt uninterrupted. But again, without some independently verifiable means to correlate specific elements of her NDE to specific physiological events, we cannot rule out this possibility, as the experience could have proceeded without her ever detecting a physiological interruption in consciousness. By definition, she would not have felt any period lacking conscious awareness. By analogy, it is conceivable that what a subject perceives to be a single, continuous dream could in fact extend across various changes in brain states, including an imperceptible period of dreamless sleep falling between two different periods of REM sleep. Consequently, that Pam’s entire NDE preceded the induction of hypothermia, or alternatively proceeded well beyond hypothermia but was interrupted by a period of unconsciousness, both remain possibilities.
[18] That Sabom’s description of the case in Light and Death is the source of these misunderstandings is evident in Stephen Braude’s comments. Despite his erroneous belief that Pam’s experience occurred during the standstill state, Braude goes on to state that in this case “it would be hasty to conclude that … mental activity clearly persisted independently of bodily activity” (Braude 274). Moreover, he concludes that in general “the case for survival receives very little independent support from OBEs, NDEs, and apparitions” (280-81). Obviously, then, Braude has no vested interest in portraying the Pam Reynolds case as strong evidence for survival of bodily death. His mistaken belief that her experience occurred during standstill was almost certainly derived directly from the source he cites—Light and Death.
[19] My timeline of Pam Reynolds’ experience during general anesthesia is derived from Sabom’s reported times in Light and Death and his commentary on this part of this paper. Numbers alone in parentheses indicate page numbers from Light and Death:
- Pam goes under general anesthesia around 7:15 AM in August 1991 (38), about 90 minutes before her OBE (185). This places her OBE at about 8:45 AM.
- By 8:40, Pam’s body is completely draped except for her head (40).
- Cooling of her blood begins at 10:50 AM (43).
- Cardiac arrest is completed at 11:05 AM (43).
- Somatosensory cortical EEG flattens at 11:10 AM (Sabom, “Commentary” 257).
- Brainstem EEG flattens at 11:24 AM (Sabom, “Commentary” 257-258).
- At 11:25 AM the bypass machine cooling her blood shuts down at 60°F so that her brain can be drained of blood and her aneurysm clipped (43).
- Warming of her blood begins at 11:30 AM (Sabom, “Commentary” 258).
- Mechanical warming of her blood ends at 12:32 PM (46).
- Postoperative anesthesia wears off around 2:10 PM. Pam wakes up to the song “Hotel California” (46).
- Sometime after 4 PM, Pam reports her NDE in the recovery room (46-47).
- Sabom interviews Pam on November 11, 1994 (186).
- Sabom transcribes the taped interview in March 1996 (186).
Gerald Woerlee offers a much more detailed timeline in his online analysis of the Pam Reynolds case on the Mortal Minds website.
[20] In his commentary Charles Tart correctly noted that the nearly 100-decibel level of the clicks in Pam’s ears, which were equivalent to “the level of sound of a full symphony orchestra playing really loud,” would have drown out any intraoperative conversations that Pam might otherwise have overheard through normal hearing (Tart, “Commentary” 253). However, as I noted in my reply to Tart’s commentary, the answers to two further questions are crucial for ruling out normal hearing as the source of Pam’s auditory recollections.
First, were clicks to measure AEPs actually being generated at the time of the conversation Pam reported? Given that the brainstem activity that AEPs are designed to measure would not falter two hours before Pam’s doctors even began to lower her body temperature, it is quite plausible that Pam’s earplugs would not have been generating clicks at the time of her auditory perceptions. Second, even if we grant the unlikely premise that her earplugs were operational at that time, we would need to know the duration of the pauses between clicks—or sets of clicks—before concluding that it was impossible for Pam to have overheard the relevant details of the intraoperative conversation in question.
Although I was regrettably unaware of the duration of the clicks at the time that I replied to Tart, I subsequently learned that there were “11.3 clicks/sec, in successive blocks of 2,000 blocks (just under 3 minutes/block)” (Kelly, Greyson, and Kelly 392n21). Although I am unaware of the exact duration of the pause (if any) between the near-3-minute blocks of clicks, I concede that it seems rather unlikely that either the relevant intraoperative comments would have coincided with such a pause, or that such a pause would have been sufficiently long to accurately reconstruct an intraoperative conversation through normal hearing. Nevertheless, I have yet to receive a definitive answer as to whether the 95 dB clicks produced to measure AEPs were actually being generated at the time of the intraoperative conversation reported by Pam.
[21] I would like to thank Richard Carrier for suggesting all of these points concerning the possibility that Pam Reynolds learned that her head would be shaved prior to her experience. I would also like to thank Gerald Woerlee for many useful comments concerning the Pam Reynolds case.
A peculiar comment by Pam suggests that she was still under the residual influence of anesthetics at the point of her veridical auditory perceptions. In her interview with Sabom, Pam recalled:
Someone said something about my veins and arteries being very small. I believe it was a female voice and that it was Dr. Murray, but I’m not sure. She was the cardiologist. I remember thinking that I should have told her about that [emphasis mine] (Sabom, “Light” 42).
As Woerlee has noted, Pam’s final sentence above suggests abnormal thinking while under the influence of anesthetics, as very few people have the slightest idea whether the arteries in either side of their groin are large enough to accommodate cardiac bypass tubing (Woerlee, “Unholy” 313).
[22] In a September 11, 2008 symposium at the United Nations, Sam Parnia announced the launch of a long-term multicenter study of veridical paranormal perception during NDEs following the successful completion of an 18-month pilot study at select hospitals in the United Kingdom. In what Parnia has dubbed the Awareness During Resuscitation (AWARE) study, target identification experiments will be carried out in the coronary care units, emergency rooms, and intensive care units of medical centers across the United States, Canada, and Europe for the next three years. During that timeframe, about 15,000 patients suffering cardiac arrest are expected to be admitted to these centers, 1500 of whom are expected to be resuscitated. Based on previous studies of NDE frequency among cardiac arrest survivors, near-death researchers anticipate that between 150 and 300 of these patients will report NDEs. The AWARE study is designed to find out whether or not any of these NDErs will be able to accurately report the complex images that appear as hidden visual targets visible only from the ceiling. Parnia explicitly states that the purpose of the study is to “settle this debate once and for all” (Taylor 24), adding that “if no one sees the pictures, it shows these experiences are illusions or false memories” (Dreaper). The study has been encouraged by both skeptics of and believers in a survivalist interpretation of NDEs.
The AWARE study will be complemented by the Brain Resuscitation Advancement International Network-1 (BRAIN-1) study, which along with AWARE will utilize an innovative “cerebral oximeter” to directly measure cerebral oxygen levels during cardiac arrest, overcoming the deficiencies of previous NDEs studies’ inferences about levels of cerebral anoxia during cardiac arrest.
[23] In his second commentary Bruce Greyson pointed out that known correlations between imagery skills and such experiences are equally well explained on the hypothesis that something leaves the body during OBEs and NDEs. That hypothesis, he notes, “also predicts that OBErs, because of the visuospatial training they receive in their OBEs, should have better imagery and visuospatial skills” (Greyson, “Correlates” 131). This is a good point. As I noted in my response, although there are independent grounds for preferring a psychophysiological explanation of such correlations over “the separation hypothesis,” they are at best merely suggestive. I noted, for instance, that techniques for inducing OBEs typically require subjects to focus on internally generated imagery. Of course, this does not provide any grounds for preferring a psychophysiological account of spontaneous OBEs and NDEs unless it can be shown that they are qualitatively the same as induced OBEs. Ultimately, if the right sorts of prospective studies were done (e.g., on the differences in spatial perspective or dream control skills during dreaming between dreamers who happen to have OBEs compared to those who do not), relevant data could be obtained (in principle if not in practice) which would decide between these two hypotheses.
[24] Notably, Harvey Irwin reports that “the majority of OBEs” terminate instantaneously rather than featuring ‘return trips’ (Irwin, “Introduction” 222).
[25] I am grateful to Oliver Carter, lecturer of English as a Foreign Language at Matsumoto University, for his research assistance and translation of Takashi Tachibana’s Rinshi Taiken.
[26] To my knowledge, my paper contains the most extensive analysis of all published contemporary non-Western NDE accounts from NDErs with limited exposure to (and thus minimal contamination from) Western culture. Nevertheless, the extreme variability in NDE content across cultures has also been independently documented in:
Belanti, John, Mahendra Perera, and Karuppiah Jagadheesan. “Phenomenology of Near-death Experiences: A Cross-cultural Perspective.” Transcultural Psychiatry. Vol. 45, No. 1 (March 2008): 121-133.
I recently learned that Gary Groth-Marnat had also made similar observations about the extent of NDE diversity across cultures as long ago as 1994:
Groth-Marnat, Gary. “Cross-Cultural Perspectives on the Near-Death Experience.” Australian Parapsychological Review. No. 19 (1994): 7-11.
[27] As Kellehear points out, Zhi-ying and Jian-xun’s data on NDEs that occurred in 1976 in China is suspect because “they did not include descriptive cases that we can analyze for content” (Kellehear 25). Moreover, they may have even offered NDErs something like a checklist of various NDE elements to choose from, contaminating their reports: “For example, although Zhi-ying and Jian-xun assert that ‘a tunnel-like dark region’ was reported by their respondents, this is, in fact, a response to a prior descriptive category offered to them” (25). Ironically, Kellehear then reports corroborating the existence of prototypical Western NDEs in China in his own 1990 study, which offered “a typical Anglo-European vignette of an NDE to a sample of 197 Chinese in Beijing” and then asked the respondents if they had ever had an experience like the one offered (26). Although 26 (or 13%) answered affirmatively, finding Chinese NDErs unexposed to the Western vignette prior to offering accounts or answering surveys (e.g., by asking about both prototypical Western NDE elements and non-NDE elements) would’ve provided far more persuasive evidence.
[28] In response to this point Allan Kellehear argued that I understate the differences between NDE content and those features “we might predict from social expectation” (Kellehear, “Culture” 148). He noted, for instance, that NDE visions have included such consciously unexpected features as colors unlike anything ever seen before, encounters with supernatural beings lacking either male or female traits, and visions of huts suspended in mid-air (149). While such imagery is undoubtedly bizarre, surely we should not assume that hallucinatory imagery is completely determined by cultural conditioning; rather, it is merely shaped by it. Extracultural factors shaping hallucinatory content include personal expectations—some conscious, some subconscious—and the unusual physiological states accompanying hallucinations. Unusual neurological conditions might very well produce experiences of novel colors, just as they can produce transient synesthetic experiences which ‘blend’ colors with other sensory modalities (e.g., seeing the ‘color’ of a particular musical tone). Moreover, bizarre visions of androgynous beings and hovering huts, which may very well call up imagery which is not consciously expected, are the norm for altered states of consciousness like dreams, and thus not particularly compelling evidence that NDEs represent sojourns into a transcendental dimension of reality.
[29] Christopher M. Moreman is one of the few commentators to explicitly acknowledge this: “While it is often claimed that NDEs have been reported throughout time, sometimes citing Plato’s story of Er as an example, it is obvious from a comparison of such ancient stories and the modern case studies that near-death experiences as they have been defined are a purely modern phenomena” (Moreman, “Proof” 49). In a recent book he also underscores the marked cross-cultural differences in NDE phenomenology, concluding: “If a common core of near-death experience can be found, it is only in the broadest of terms” (Moreman, “Beyond” 264). As I have shown, there is little evidence that prototypical Western NDE motifs feature in minimally ‘contaminated’ non-Western NDE case studies.
[30] Though this encounter with a mythological centaur followed a man’s electrocution and included his decision to return to life because he “had too many things to do,” in his commentary William Serdahely suggested that it may have been a hallucination but only been misidentified as an NDE (Serdahely, “Commentary” 51). This raises the issue of when an experience should or should not be defined as an NDE when a reliable psychological measure like the Greyson NDE Scale has not been applied.
[31] In his commentary William Serdahely noted that it is possible that this woman actually left her body during her NDE, but that her NDE was followed by a distinct hallucinatory experience immediately after returning to her body (Serdahely, “Commentary” 52).
[32] Janice Holden’s commentary offers a similar ad hoc explanation for the discovery of NDEs featuring living persons in an ostensibly transcendental realm: “a transcendent benevolent entity seeking to encourage ongoing physical existence might most effectively appear in the form of a living person known to the NDEr” (Holden, “Heaven” 39). As I noted in my response, however, that NDEs are hallucinations is a simpler and far more plausible explanation for encounters with living persons during NDEs than the alternative of impersonation by “transcendent entities,” particularly since the reality of any transcendent entities is contentious, whereas the reality of hallucinations is not. What makes Holden’s alternative particularly ad hoc is that it renders a survivalist interpretation of NDEs unfalsifiable, as any imaginable encounter during NDEs, such as an encounter with a mythological creature, could be explained away in terms of transcendental impersonation. Moreover, the only apparent reason to posit transcendental impersonation in these cases is to save a survivalist interpretation of them; after all, no one factors in the bare possibility that transcendental impersonation may have occurred during NDE encounters that lack overt hallucinatory features.
[33] Tart never says this explicitly, but it is implied by his failure to acknowledge any alternative possibilities for why someone would reject survival of bodily death or deny that NDEs are evidence for survival.
[34] A survey conducted by Richard Carrier indicates that most materialists believe that materialism can be falsified—and even go so far as to offer examples of possible falsifying evidence—but that, as a matter of fact, no unambiguous evidence falsifying materialism has ever been produced. Thus Tart’s implication that materialists don’t recognize that materialism “should be treated like any scientific theory” distorts the reality of the situation. In fact, most materialists do recognize this, but fail to be convinced that the inconclusive parapsychological evidence Tart relies on has actually falsified it. To suggest otherwise it to attack a caricature of contemporary materialists for polemical purposes. See Richard Carrier’s “Defending Naturalism as a Worldview: A Rebuttal to Michael Rea’s World Without Design.” Carrier’s discussion is specifically about naturalism, but naturalism can be seen as roughly equivalent to materialism for our purposes (strictly speaking, materialism is a specific kind of naturalism, but the evidence that would falsify naturalism would also falsify materialism). Carrier’s survey of what naturalists (and the materialists among them) really believe is discussed at length in the section “A Brief Ethnography of Contemporary Naturalism.”
References
Abanes, Richard. Journey Into the Light: Exploring Near-Death Experiences. Grand Rapids, MI: Baker Books, 1996.
Abramovitch, Henry. “An Israeli Account of a Near-Death Experience: A Case Study of Cultural Dissonance.” Journal of Near-Death Studies. Vol. 6, No. 3 (Spring 1988): 175-184.
Alvarado, Carlos S. “Out-of-Body Experiences.” In The Varieties of Anomalous Experience: Examining the Scientific Evidence, ed. Etzel Cardeña, Steven Jay Lynn, and Stanley Krippner. Washington, DC: American Psychological Association, 2000: 183-218.
Alvarado, Carlos S. and Nancy L. Zingrone. “Individual Differences in Aura Vision: Relationships to Visual Imagery and Imaginative-Fantasy Experiences.” European Journal of Parapsychology. Vol. 10 (1994): 1-30.
Athappilly, Geena K., Bruce Greyson, and Ian Stevenson. “Do Prevailing Societal Models Influence Reports of Near-Death Experiences? A Comparison of Accounts Reported Before and After 1975.” Journal of Nervous and Mental Disease. Vol. 194, No. 3 (March 2006): 218-222.
Atwater, Phyllis M. H. “Another look… The experience/The experiencer.” Vital Signs. Vol. 19, No. 2 (2000): 12-13.
Badham, Paul. “Religious and Near-Death Experience in Relation to Belief in a Future Life.” Mortality. Vol. 2, No. 1 (March 1997): 7-21.
Bailey, Lee W. “A ‘Little Death’: The Near-Death Experience and Tibetan Delogs.” Journal of Near-Death Studies. Vol. 19, No. 3 (Spring 2001): 139-159.
Bardy, Ali Henri. “Correspondence: Near-Death Experiences.” Lancet. Vol. 359, Issue 9323 (June 15, 2002): 2116.
Becker, Carl B. “The Centrality of Near-Death Experiences in Chinese Pure Land Buddhism.” Anabiosis: The Journal of Near-Death Studies. Vol. 1, No. 2 (December 1981): 154-170.
Becker, Carl B. “The Pure Land Revisited: Sino-Japanese Meditations and Near-Death Experiences of the Next World.” Anabiosis: The Journal of Near-Death Studies. Vol. 4, No. 1 (Spring 1984): 51-68.
Beloff, John. “Is There Anything Beyond Death? A Parapsychologist’s Summation.” In Immortality, ed. Paul Edwards. New York, NY: Macmillan, 1992: 259-268.
Benson, Herbert, Jeffery A. Dusek, Jane B. Sherwood, Peter Lam, Charles F. Bethea, William Carpenter, Sidney Levitsky, Peter C. Hill, Donald W. Clem Jr., Manoj K. Jain, David Drumel, Stephen L. Kopecky, Paul S. Mueller, Dean Marek, Sue Rollins, and Patricia L. Hibberd. “Study of the Therapeutic Effects of Intercessory Prayer (STEP) in Cardiac Bypass Patients: A Multicenter Randomized Trial of Uncertainty and Certainty of Receiving Intercessory Prayer.” American Heart Journal. Vol. 151, No. 4 (April 2006): 934-942.
Berndt, Ronald M. and Catherine H. Berndt. The Speaking Land: Myth and Story in Aboriginal Australia. Harmondsworth, England: Penguin, 1999.
Blackmore, Susan. Beyond the Body: An Investigation of Out-of-the-Body Experiences. Chicago, IL: Academy Chicago Publishers, 1992.
Blackmore, Susan. Dying to Live: Near-Death Experiences. Buffalo, NY: Prometheus Books, 1993.
Blackmore, Susan. “Near-Death Experiences in India: They Have Tunnels Too.” Journal of Near-Death Studies. Vol. 11, No. 4 (Summer 1993): 205-217.
Blackmore, Susan. “A Postal Survey of OBEs and Other Experiences.” Journal of the Society for Psychical Research. Vol. 52, No. 796 (February 1984): 225-244.
Blackmore, Susan. “Where Am I? Perspectives in Imagery and the Out-of-Body Experience.” Journal of Mental Imagery. Vol. 11, No. 2 (Summer 1987): 53-66.
Blanke, Olaf, Stéphanie Ortigue, Theodor Landis, and Margitta Seeck. “Neuropsychology: Stimulating Illusory Own-Body Perceptions.” Nature. Vol. 419, No. 6904 (19 September 2002): 269-270.
Bonenfant, Richard J. “A Comparative Study of Near-Death Experience and Non-Near-Death Experience Outcomes in 56 Survivors of Clinical Death.” Journal of Near-Death Studies. Vol. 22, No. 3 (Spring 2004): 155-178.
Braithwaite, Jason J. “Towards a Cognitive Neuroscience of the Dying Brain.” The Skeptic (UK). Vol. 21, No. 2 (Summer 2008): 8-16.
Bremmer, Jan N. The Rise and Fall of the Afterlife. New York, NY: Routledge, 2002.
Bressloff, Paul C., Jack D. Cowan, Martin Golubitsky, Peter J. Thomas, and Matthew C. Wiener. “What Geometric Visual Hallucinations Tell Us About the Visual Cortex.” Neural Computation. Vol. 14, No. 3 (March 2002): 473-491.
Braude, Stephen. Immortal Remains: The Evidence for Life After Death. Lanham, MD: Rowman & Littlefield Publishers, 2003.
Brinkley, Dannion and Paul Perry. Saved by the Light: The True Story of a Man Who Died Twice and the Profound Revelations He Received. New York, NY: Villard Books, 1994.
Britton, Willoughby B. and Richard R. Bootzin. “Near-Death Experiences and the Temporal Lobe.” Psychological Science. Vol. 15, No. 4 (April 2004): 254-258.
Bünning, Silvia and Olaf Blanke. “The Out-of Body Experience: Precipitating Factors and Neural Correlates.” In The Boundaries of Consciousness: Neurobiology and Neuropathology, ed. Steven Laureys. New York, NY: Elsevier Science, 2005: 331-350.
Buzzi, Giorgio. “Correspondence: Near-Death Experiences.” Lancet. Vol. 359, Issue 9323 (June 15, 2002): 2116-2117.
Clark, Kimberly. “Clinical Interventions with Near-Death Experiencers.” In The Near-Death Experience: Problems, Prospects, Perspectives, ed. Bruce Greyson and Charles P. Flynn. Springfield, IL: Charles C. Thomas Publisher, 1984: 242-255.
Cook, Anne M. and Harvey J. Irwin. “Visuospatial Skills and the Out-of-Body Experience.” Journal of Parapsychology. Vol. 47, No. 1 (March 1983): 23-35.
Corcoran, Diane, Janice Miner Holden, and Debbie James. “The Near Death Experience: 30 Years of Research.” Association for Transpersonal Psychology 2005 Conference: Spirit in Dying, Berkeley, CA, June 10, 2005.
Council, James R., Bruce Greyson, and Kenneth D. Huff. “Fantasy-Proneness, Hypnotizability, and Reports of Paranormal Experiences.” American Psychological Association Annual Convention, Washington, DC, August 1986.
Counts, Dorothy Ayers. “Near-Death and Out-of-Body Experiences in a Melanesian Society.” Anabiosis: The Journal of Near-Death Studies. Vol. 3, No. 2 (December 1983): 115-135.
Crookall, Robert. More Astral Projections: Analyses of Case Histories. London: Aquarian Press, 1964.
Devinsky, Orrin, Edward Feldmann, Kelly Burrowes, and Edward Bromfield. “Autoscopic Phenomena with Seizures.” Archives of Neurology. Vol. 46, No. 10 (October 1989): 1080-1088.
Drab, Kevin J. “The Tunnel Experience: Reality or Hallucination?” Anabiosis: The Journal of Near-Death Studies. Vol. 1, No. 2 (December 1981): 126-152.
Dreaper, Jane. “Study Into Near-Death Experiences.” BBC News. September 18, 2008. Health section. <http://news.bbc.co.uk/1/hi/health/7621608.stm>.
Ebbern, Hayden, Sean Mulligan, and Barry Beyerstein, “Maria’s Near-Death Experience: Waiting for the Other Shoe to Drop.” Skeptical Inquirer. Vol. 20, No. 4 (July/August 1996): 27-33.
Fenwick, Peter. “Commentary on ‘Near-Death Experiences with Hallucinatory Features’.” Journal of Near-Death Studies. Vol. 26, No. 1 (Fall 2007): 43-49.
Fenwick, Peter and Elizabeth Fenwick. The Truth in the Light: An Investigation of Over 300 Near-Death Experiences. New York, NY: Berkley Books, 1997.
Floyd, Keith. “ECT: TNT or TLC? A Near-Death Experience Triggered by Electroconvulsive Therapy.” Journal of Near-Death Studies, Vol. 14, No. 3 (Spring 1996): 187-196.
Fox, Mark. Religion, Spirituality and the Near-Death Experience. New York, NY: Routledge, 2003.
French, Christopher C. “Near-Death Experiences in Cardiac Arrest Survivors.” In The Boundaries of Consciousness: Neurobiology and Neuropathology, ed. Steven Laureys. New York, NY: Elsevier Science, 2005: 351-367.
Gabbard, Glen O., Stuart W. Twemlow, and Fowler C. Jones. “Do ‘Near-Death Experiences’ Occur Only Near Death?” Journal of Nervous and Mental Disease. Vol. 169, No. 6 (June 1981): 374-377.
Gabbard, Glen O. and Stuart W. Twemlow. “Do ‘Near-Death Experiences’ Occur Only Near Death?—Revisited.” Journal of Near-Death Studies. Vol. 10, No. 1 (Fall 1991): 41-47.
Gallup Jr., George. The Gallup Poll: Public Opinion 1991. Wilmington, DE: Scholarly Resources, 1992.
Glicksohn, Joseph. “Belief in the Paranormal and Subjective Paranormal Experience.” Personality and Individual Differences. Vol. 11, No. 7 (1990): 675-683.
Gómez-Jeria, Juan S. “A Near-Death Experience Among the Mapuche People.” Journal of Near-Death Studies. Vol. 11, No. 4 (Summer 1993): 219-222.
Green, J. Timothy. “Near-Death Experiences in a Chammorro Culture.” Vital Signs. Vol. 4, No. 1/2 (1984): 6-7.
Greyson, Bruce. “Comments on ‘Does Paranormal Perception Occur in Near-Death Experiences?’.” Journal of Near-Death Studies. Vol. 25, No. 4 (Summer 2007): 237-244.
Greyson, Bruce. “Comments on ‘Psychophysiological and Cultural Correlates Undermining a Survivalist Interpretation of Near-Death Experiences’.” Journal of Near-Death Studies. Vol. 26, No. 2 (Winter 2007): 127-145.
Greyson, Bruce. “Consistency of Near-Death Experience Accounts over Two Decades: Are Reports Embellished over Time?” Resuscitation. Vol. 73, Issue 3 (June 2007): 407-411.
Greyson, Bruce. “Near-Death Experiences.” In The Varieties of Anomalous Experience: Examining the Scientific Evidence, ed. Etzel Cardeña, Steven Jay Lynn, and Stanley Krippner. Washington, DC: American Psychological Association, 2000: 315-352.
Greyson, Bruce and Nancy Evans Bush. “Distressing Near-Death Experiences.” Psychiatry. Vol. 55, No. 1 (1992): 95-110.
Greyson, Bruce and Ian Stevenson. “The Phenomenology of Near-Death Experiences.” American Journal of Psychiatry. Vol. 137, No. 10 (October 1980): 1193-1196.
Greyson, Bruce, Janice M. Holden, and J. Paul Mounsey. “Failure to Elicit Near-Death Experiences in Induced Cardiac Arrest.” Journal of Near-Death Studies. Vol. 25, No. 2 (Winter 2006): 85-98.
Grossman, Neal. “Four Errors Commonly Made by Professional Debunkers [Letter].” Journal of Near-Death Studies. Vol. 26, No. 3 (Spring 2008): 231-238.
Grossman, Neal. “Who’s Afraid of Life After Death? [Guest Editorial].” Journal of Near-Death Studies. Vol. 21, No. 1 (Fall 2002): 5-24.
Groth-Marnat, Gary and Roger Summers. “Altered Beliefs, Attitudes, and Behaviors Following Near-Death Experiences.” Journal of Humanistic Psychology. Vol. 38, No. 3 (July 1998): 110-125.
Hadfield, Peter. “Japanese Find Death a Depressing Experience.” New Scientist Vol. 132, Issue 1797 (November 30, 1991): 11.
Hampe, Johann Christophe. To Die is Gain: The Experience of One’s Own Death. London: Darton, Longman & Todd, 1979.
Harris, Barbara and Lionel Bascom. Full Circle: The Near-Death Experience and Beyond. New York, NY: Pocket Books, 1990.
Holden, Janice M. “More Things in Heaven and Earth: A Response to ‘Near-Death Experiences with Hallucinatory Features’.” Journal of Near-Death Studies. Vol. 26, No. 1 (Fall 2007): 33-42.
Holden, Janice M. and Leroy Joesten. “Near-Death Veridicality Research in the Hospital Setting: Problems and Promise.” Journal of Near-Death Studies. Vol. 9, No. 1 (Fall 1990): 45-54.
Holden, Janice M., Jeff Long, and Jason MacLurg. “Out-of-Body Experiences: All in the Brain?” Journal of Near-Death Studies. Vol. 25, No. 2 (Winter 2006): 99-107.
Hunt, Harry T., Arlene Gervais, Sheryl Shearing-Johns, and Fred Travis. “Transpersonal Experiences in Childhood: An Exploratory Empirical Study of Selected Adult Groups.” Perceptual and Motor Skills. Vol. 75, Issue 3, Pt 2 (December 1992): 1135-1153.
Irwin, Harvey J. “The Disembodied Self: An Empirical Study of Dissociation and the Out-of-Body Experience.” Journal of Parapsychology. Vol. 64, No. 3 (September 2000): 261-277.
Irwin, Harvey J. Flight of Mind: A Psychological Study of the Out-of-Body Experience. Metuchen, NJ: Scarecrow Press, 1985.
Irwin, Harvey J. “Images of Heaven.” Parapsychology Review. Vol. 18, No. 1 (January/February 1987): 1-4.
Irwin, Harvey J. An Introduction to Parapsychology (3rd ed). Jefferson, NC: McFarland and Company, 1999.
Irwin, Harvey J. “The Near-Death Experience as a Dissociative Phenomenon: An Empirical Assessment.” Journal of Near-Death Studies. Vol. 12, No. 2 (Winter 1993): 95-103.
Irwin, Harvey J. “Parapsychological Phenomena and the Absorption Domain.” Journal of the American Society for Psychical Research. Vol. 79, No. 1 (January 1985): 1-11.
Irwin, Harvey J. “Perceptual Perspective of Visual Imagery in OBEs, Dreams, and Reminiscence.” Journal of the Society for Psychical Research. Vol. 53, No. 802 (January 1986): 210-217.
Irwin, Harvey J. “Review of Mindsight: Near-Death and Out-of-Body Experiences in the Blind.” Journal of Parapsychology. Vol. 64, No. 1 (March 2000): 107-113.
Jansen, Karl. Ketamine: Dreams and Realities. Sarasota, FL: Multidisciplinary Association for Psychedelic Studies, 2001.
Joint Commission on the Accreditation of Healthcare Organizations (JCAHO). “Preventing and Managing the Impact of Anesthesia Awareness.” Joint Commission Perspectives. Vol. 24, No. 12 (December 2004): 10-11.
Kellehear, Allan. “Culture and the Near-Death Experience: Comments on Keith Augustine’s ‘Psychophysiological and Cultural Correlates Undermining a Survivalist Interpretation of Near-Death Experiences’.” Journal of Near-Death Studies. Vol. 26, No. 2 (Winter 2007): 147-153.
Kellehear, Allan. Experiences Near Death: Beyond Medicine and Religion. New York, NY: Oxford University Press, 1996.)
Kellehear, Allan, Patrick Heaven, and Jia Gao. “Community Attitudes Toward Near-Death Experiences: A Chinese Study.” Journal of Near-Death Studies. Vol. 8, No. 3 (March 1990): 163-173.
Kelly, Emily Williams, Bruce Greyson, and Edward F. Kelly. “Unusual Experiences Near Death and Related Phenomena.” In Irreducible Mind: Toward a Psychology for the 21st Century, ed. Edward F. Kelly, Emily Williams Kelly, Adam Crabtree, Alan Gauld, Michael Grosso, and Bruce Greyson. Lanham, MD: Rowman and Littlefield, 2006: 367-421.
Kohr, Richard L. “Near-Death Experiences, Altered States, and Psi Sensitivity.” Anabiosis: The Journal of Near-Death Studies. Vol. 3, No. 2 (December 1983): 157-176.
Krishnan, V. “Near-Death Experiences: Evidence For Survival?” Anabiosis: The Journal of Near-Death Studies. Vol. 5, No. 1 (1985): 21-38.
Lange, Rense, Bruce Greyson, and James Houran. “A Rasch Scaling Validation of a ‘Core’ Near-Death Experience.” British Journal of Psychology. Vol. 95, Pt. 2 (May 2004): 161-177.
Lawrence, Madelaine. In a World of Their Own: Experiencing Unconsciousness. Westport, CT: Praeger Publishers, 1997.
Lester, David. Is There Life After Death? An Examination of the Empirical Evidence. Jefferson, NC: McFarland and Company, 2005.
Levine, Art. “Tunnel Visions.” CityLink. March 19, 2003. Cover Story (Box: “Past Imperfect”).
Lindley, James H., Sethryn Bryan, and Bob Conley. “Near-Death Experiences in a Pacific Northwest American Population: The Evergreen Study.” Anabiosis: The Journal of Near-Death Studies. Vol. 1, No. 2 (1981): 104-124.
MacMillan, R. L. and K. W. G. Brown. “Cardiac Arrest Remembered [Letter].” Canadian Medical Association Journal. Vol. 104, No. 10 (May 22, 1971): 889-890.
Makarec, Katherine and Michael A. Persinger. “Temporal Lobe Signs: Electroencephalographic Validity and Enhanced Scores in Special Populations.” Perceptual and Motor Skills. Vol. 60, No. 3 (June 1985): 831-842.
Mauro, James. “Bright Lights, Big Mystery.” Psychology Today. July/August 1992: 54-57, 80-82.
McClenon, James. “Kongo Near-Death Experiences: Cross-Cultural Patterns.” Journal of Near-Death Studies. Vol. 25, No. 1 (Fall 2006): 21-34.
McClenon, James. “Near-Death Folklore in Medieval China and Japan: A Comparative Analysis.” Asian Folklore Studies. Vol. 50, No. 2 (1991): 319-342.
McCreery, Charles and Gordon Claridge. “Out-of-the-Body-Experiences and Personality.” Journal of the Society for Psychical Research. Vol. 60, No. 838 (January 1995): 129-148.
McCreery, Charles and Gordon Claridge. “A Study of Hallucination in Normal Subjects: I. Self-Report Data.” Personality and Individual Differences. Vol. 21, No. 5 (November 1996): 739-747.
Moody, Raymond. Life After Life: The Investigation of a Phenomenon—Survival of Bodily Death. Covington, CA: Mockingbird Books, 1975.
Moreman, Christopher M. Beyond the Threshold: Afterlife Beliefs and Experiences in World Religions. Lanham, MD: Rowman & Littlefield Publishers, 2008.
Moreman, Christopher M. “Is There Proof of a Life After Death? An Overview of the Evidence from Psychical Research.” Journal of Religion and Culture. Vol. 15 (2002/2003): 38-61.
Morse, Melvin. “Near Death Experiences and Death-Related Visions in Children: Implications for the Clinician.” Current Problems in Pediatrics, Vol. 24, No. 2 (February 1994): 55-83.
Morse, Melvin and Paul Perry. Parting Visions: Uses and Meanings of Pre-Death, Psychic, and Spiritual Experiences. New York, NY: Villard Books, 1994.
Morse, Melvin and Paul Perry. Transformed by the Light: The Powerful Effect of Near-Death Experiences on People’s Lives. New York, NY: Villard Books, 1992.
Murphy, Todd. “Eleven Thai Near-Death Experiences.” Altered States Website. 1999. 23 January 2006 <http://www.altered-states.net/barry/newsletter224/ndethai1.htm>.
Murphy, Todd. “Near-Death Experiences in Thailand.” Journal of Near-Death Studies. Vol. 19, No. 3 (Spring 2001): 161-178.
Murray, Craig and Jezz Fox. “The Out-of-Body Experience and Body Image: Differences Between Experients and Nonexperients.” Journal of Nervous and Mental Disease. Vol. 193, No. 1 (January 2005): 70-72.
Myers, Susan A., Harvey R. Austrin, J. Thomas Grisso, and Richard C. Nickeson. “Personality Characteristics as Related to the Out-of-Body Experience.” Journal of Parapsychology. Vol. 47, No. 2 (June 1983): 131-144.
National Institute of Neurological Disorders and Stroke (NINDS). “Neurological Diagnostic Tests and Procedures.” National Institutes of Health Publication No. 05-5380 (March 2005).
Neppe, Vernon M. “‘Out-of-Body Experiences’ (OBEs) and Brain Localisation. A Perspective.” Australian Journal of Parapsychology. Vol. 2, No. 2 (2002): 85-96.
Noyes, Russell and Roy Kletti. “Depersonalization in the Face of Life Threatening Danger: A Description.” Psychiatry. Vol. 39, No. 1 (February 1976): 19-27.
Osis, Karlis and Erlendur Haraldsson. At the Hour of Death: The Results of Research on Over 1000 Afterlife Experiences. New York, NY: Avon Books, 1977.
Owens, Justine E., Emily Williams Cook, and Ian Stevenson. “Features of ‘Near-Death Experience’ in Relation to Whether or Not Patients were Near Death.” Lancet. Vol. 336, Issue 8724 (November 10, 1990): 1175-1177.
Parnia, Sam, D. G. Waller, R. Yeates, and Peter Fenwick. “A Qualitative and Quantitative Study of the Incidence, Features and Aetiology of Near Death Experiences in Cardiac Arrest Survivors.” Resuscitation. Vol. 48, No. 2 (February 2001): 149-156.
Pasricha, Satwant. “A Systematic Survey of Near-Death Experiences in South India.” Journal of Scientific Exploration. Vol. 7, No. 2 (Summer 1993): 161-171.
Pasricha, Satwant and Ian Stevenson. “Near-Death Experiences in India: A Preliminary Report.” Journal of Nervous and Mental Disease. Vol. 174, No. 3 (March 1986): 165-174.
Richards, Pauline and Michael A. Persinger. “Temporal Lobe Signs, the Dissociative Experiences Scale and the Hemispheric Quotient.” Perceptual and Motor Skills. Vol. 72, No. 3 (June 1991): 1139-1142.
Ring, Kenneth. “Solving the Riddle of Frightening Near-Death Experiences: Some Testable Hypotheses and a Perspective Based on A Course in Miracles.” Journal of Near-Death Studies. Vol. 13, No. 1 (Fall 1994): 5-23.
Ring, Kenneth. “Religious Wars in the NDE Movement: Some Personal Reflections on Michael Sabom’s Light & Death.” Journal of Near-Death Studies. Vol. 18, No. 4 (Summer 2000): 215-244.
Ring, Kenneth and Sharon Cooper. Mindsight: Near-Death and Out-of-Body Experiences in the Blind. Palo Alto, CA: William James Center for Consciousness Studies, 1999.
Ring, Kenneth and Sharon Cooper. “Near-Death and Out-of-Body Experiences in the Blind: A Study of Apparent Eyeless Vision.” Journal of Near-Death Studies. Vol. 16, No. 2 (December 1997): 101-147.
Ring, Kenneth and Madelaine Lawrence. “Further Evidence for Veridical Perception During Near-Death Experiences.” Journal of Near-Death Studies. Vol. 11, No. 4 (Summer 1993): 223-229.
Ring, Kenneth and Christopher J. Rosing. “The Omega Project: An Empirical Study of the NDE-Prone Personality.” Journal of Near-Death Studies. Vol. 8, No. 4 (June 1990): 211-239.
Rodabough, Tillman. “Near-Death Experiences: An Examination of the Supporting Data and Alternative Explanations.” Death Studies. Vol. 9, No. 2 (1985): 95-113.
Rommer, Barbara. Blessing in Disguise: Another Side of the Near-Death Experience. St. Paul, MN: Llewellyn, 2000.
Sabom, Michael B. “Commentary on ‘Does Paranormal Perception Occur in Near-Death Experiences?’.” Journal of Near-Death Studies. Vol. 25, No. 4 (Summer 2007): 257-260.
Sabom, Michael B. Recollections of Death: A Medical Investigation. New York, NY: Harper & Row, 1982.
Sabom, Michael B. Light and Death: One Doctor’s Fascinating Account of Near-Death Experiences. Grand Rapids, MI: Zondervan Publishing House, 1998.
Sabom, Michael B. “The Shadow of Death (Part One).” Christian Research Journal. Vol. 26, No. 2 (2003): 5-8.
Sartori, Penny. “A Prospective Study of NDEs in an Intensive Therapy Unit.” Christian Parapsychologist. Vol. 16, No. 2 (June 2004): 34-40.
Schorer, C. E. “Two Native North American Near-Death Experiences.” Omega: Journal of Death and Dying. Vol. 16, No. 2 (1985): 111-113.
Serdahely, William. “Commentary on Keith Augustine’s Paper.” Journal of Near-Death Studies. Vol. 26, No. 1 (Fall 2007): 51-53.
Serdahely, William. “Variations from the Prototypic Near-Death Experience: The ‘Individually Tailored’ Hypothesis.” Journal of Near-Death Studies. Vol. 13, No. 3 (Spring 1995): 185-196.
Singh, Ajai R., V. N. Bagadia, P. V. Pradhan, and V. N. Acharya. “Death, Dying and Near Death Experience.” Indian Journal of Psychiatry. Vol. 30, No. 3 (July 1988): 299-306.
Stevenson, Ian and Emily Williams Cook. “Involuntary Memories During Severe Physical Illness or Injury.” Journal of Nervous and Mental Disease. Vol. 183, No. 7 (July 1995): 452-458.
Stevenson, Ian, Emily Williams Cook, and Nicholas McClean-Rice. “Are Persons Reporting ‘Near-Death Experiences’ Really Near Death? A Study of Medical Records.” Omega: Journal of Death and Dying. Vol. 20, No. 1 (1989-90): 45-54.
Tachibana, Takashi. Rinshi Taiken [Near Death Experience] (2 vols.). Tokyo, Japan: Bungei Shunjusha, 2000.
Tart, Charles. “Commentary on ‘Does Paranormal Perception Occur in Near-Death Experiences?’.” Journal of Near-Death Studies. Vol. 25, No. 4 (Summer 2007): 251-256.
Tart, Charles. “Six Studies of Out-of-Body Experiences.” Journal of Near-Death Studies. Vol. 17, No. 2 (Winter 1998): 73-99.
Taylor, Jerome. “Is It Possible to Have an ‘Out-of-Body Experience’?” The Independent. September 19, 2008. Science section, page 24.
Tong, Frank. “Out-of-Body Experiences: From Penfield to Present.” Trends in Cognitive Science. Vol. 7, No. 3 (March 2003): 104-106.
Twemlow, Stuart W. and Glen O. Gabbard. “The Influence of Demographic/Psychological Factors and Preexisting Conditions on the Near-Death Experience.” Omega: Journal of Death and Dying. Vol. 15, No. 3 (1984): 223-235.
Twemlow, Stuart W., Glen O. Gabbard, and Lolafaye Coyne. “A Multivariate Method for the Classification of Preexisting Near-Death Conditions.” Anabiosis: The Journal of Near-Death Studies. Vol. 2, No. 2 (December 1982): 132-139.
van Lommel, Pim, Ruud van Wees, Vincent Meyers, and Ingrid Elfferich. “Near-Death Experiences in Survivors of Cardiac Arrest: A Prospective Study in the Netherlands.” Lancet. Vol. 358, Issue 9298 (December 15, 2001): 2039-2045.
Vuilleumier, P., P. A. Despland, G. Assal, and F. Regli. “Voyages Astraux et Hors du Corps: Héautoscopie, Extase et Hallucinations Expérientielles d’Origine épileptique [Out-of-Body and Astral Journeys: Heautoscopy, Ecstasis and Experimental Hallucinations of Epileptic Origin].” Revue Neurologique. Vol. 153, No. 2 (March 1997): 115-119.
Wade, Jenny. “In a Sacred Manner We Died: Native American Near-Death Experiences.” Journal of Near-Death Studies. Vol. 22, No. 2 (Winter 2003): 83-116.
Wilson, Sheryl C. and Theodore X. Barber. “The Fantasy-Prone Personality: Implications for Understanding Imagery, Hypnosis, and Parapsychological Phenomena.” In Imagery: Current Theory, Research, and Application, ed. A. A. Sheikh. New York, NY: Wiley, 1983: 340-387.
Woerlee, G. M. “Cardiac Arrest and Near-Death Experiences.” Journal of Near-Death Studies. Vol. 22, No. 4 (Summer 2004): 235-249.
Woerlee, G. M. “Pam Reynolds’ Near Death Experience.” Mortal Minds Website. February 26, 2005. 28 November 2007 <http://www.mortalminds.woerlee.org/reynolds.html>.
Woerlee, G. M. “An Anaesthesiologist Examines the Pam Reynolds Story. Part Two: The Experience.” The Skeptic (UK). Vol. 18, No. 2 (Summer 2005): 16-20.
Woerlee, G. M. The Unholy Legacy of Abraham. Leicester, UK: Matador, 2008.
Zaleski, Carol. Otherworld Journeys: Accounts of Near-Death Experience in Medieval and Modern Times. New York, NY: Oxford University Press, 1987.
Zaleski, Carol. The Life of the World to Come: Near-Death Experience and Christian Hope. New York, NY: Oxford University Press, 1996.
Zhi-ying, Feng and Liu Jian-xun. “Near-Death Experiences Among Survivors of the 1976 Tangshan Earthquake.” Journal of Near-Death Studies. Vol. 11, No. 1 (Fall 1992): 39-48.
Copyright ©2008 Keith Augustine. The electronic version is copyright ©2008 by Internet Infidels, Inc. with the written permission of Keith Augustine. All rights reserved.