
(2009)
Introduction
Many years ago I took part in a debate about whether near-death experiences (NDEs) provide compelling evidence for life after death, or are simply manifestations of brain function. I took the skeptical position that these experiences are the products of brain function. During the question and answer period, a young woman stood up and stated that she believed that NDEs were proof of Christianity, for during their experiences many NDErs found themselves in the Heaven described by the Bible, where they not only saw their deceased relatives, but also saw Jesus, Christian saints, and sometimes even God. NDErs would not see these things, she argued, and could not have had such similar experiences, unless Christianity was the one true faith. After she sat down she was treated to warm approval and support from the other members of the Christian Students’ Union. Indeed, after having heard both this statement and the witness of those who had undergone an NDE, the general opinion of the audience seemed to be that NDEs truly provided proof not only of life after death, but of the reality of a “living” Jesus and a loving God, and of the truth of Christianity. I was defeated. Belief had prevailed over science and logic.
Raymond Moody brought the NDE phenomenon to the attention of the general public with the publication of his popular book Life After Life in 1975 (Moody 1975). This was a small book describing the incredible and profoundly moving experiences of those who apparently returned to life after having undergone a period of what was termed “clinical death.” There was considerable public and scientific response to the book. Many people have taken these experiences as proof of life after death, and some even believe that they confirm the truth of their religion. Since the publication of Life After Life several investigators have performed outstanding studies of NDEs, documenting their incidence and properties (Rawlings 1979; Sabom 1983; Grey 1986; Osis and Haraldsson 1986; Lempert, Bauer, Schmidt 1994; van Lommel et al. 2001; Parnia et al. 2001; Greyson 2003). In addition, the International Association of Near-Death Studies (IANDS) was formed to further the scientific study of these experiences, and even publishes a very good scientific journal reporting studies on this subject—The Journal of Near-Death Studies. But what is the result of more than 30 years of public interest and scientific endeavor?
The answer to this question is disappointing. Many promising lines of research have not even been touched upon, while others have not been followed up. The general public continues to enthusiastically express wonder, awe, and belief in the supernatural nature of these experiences. This belief is encouraged by popular books written by medical practitioners using their authority as physicians to bolster readers’ perceptions of NDEs as genuine medical and scientific confirmation of life after death (Rawlings 1979; Osis and Haraldsson 1986; Sabom 1998; Beauregard and O’Leary 2007; van Lommel 2007). Although these books contain observational studies of NDEs which are quite good, their authors invariably entice readers to accept uncritical supernaturalistic or paranormal explanations for NDEs. Moreover, many good studies languish unread by mainstream scientists, and ignored in popular science books and scientific journals, because of the aura of popular New Age mysticism surrounding them.
This is a pity, for some of these studies reveal unexplored gaps, veritable black holes of ignorance simply begging to be investigated. This article will consider some of them. What follows, then, is a select inventory of the gaps in our current knowledge of the causes and genesis of NDEs, intended to provoke thought and further study, rather than pretending to be a complete review of the deficiencies in our knowledge of the NDE. Highlighting these fascinating gaps in our knowledge should provide an impetus for future research to reveal the true nature of these wondrous experiences—experiences which illuminate the deepest reaches of the human psyche.
Defining the Near-Death Experience
As with all analyses, I will start by defining that which is being discussed. The characteristics of the NDE as defined by Moody in 1975 (Moody 1975) are still employed by many NDE researchers. Moody defined NDEs as consisting of some combination of the following group of experiences:
- A feeling of peace and calm.
- The sense that death is imminent or has occurred.
- Hearing a noise or music.
- The experience of entering a tunnel or darkness.
- The experience of leaving one’s body.
- Meeting figures, strangers, deities, or deceased relatives.
- Meeting a being of light, or entering into a brightness or light.
- A review of the major events of one’s life.
- The experience of encountering a border, or limit, the passing of which means certain death.
- The conscious decision to return to the body.
These are the elements that NDErs most commonly reported in Moody’s collection of NDE accounts. Kenneth Ring (Ring 1980) subsequently proposed a more streamlined, five-element “core NDE” because his selected elements were the most common ones in his collection of NDE accounts:
- Peace, and a sense of well-being.
- Separation from the body.
- Entering the darkness or tunnel.
- Seeing the light.
- Entering the light.
The more of these elements experienced during an NDE, the more “profound” or “deeper” Ring classified it. As with Moody’s definition, these elements were only selected because they were most frequently encountered in NDErs’ reports. But their common occurrence in NDE accounts does not necessarily indicate that these elements are components of the NDE itself. So Bruce Greyson set out to determine which elements were essential to the experience itself through cluster analysis (Greyson 1983). Greyson found that “time standing still,” experiences of light, and experiences of tunnels or darkness were not genuine components of the NDE itself. He consequently constructed a 16-point Near-Death Experience Scale containing only elements related to the experience itself. This scale provides the most reliable definition of the NDE to date, and has been validated in its use for over 20 years (Lange, Greyson, and Houran 2004). The elements of the Greyson Near-Death Experience Scale are further subdivided into cognitive, affective, paranormal, and transcendental experiences (Greyson 1983).
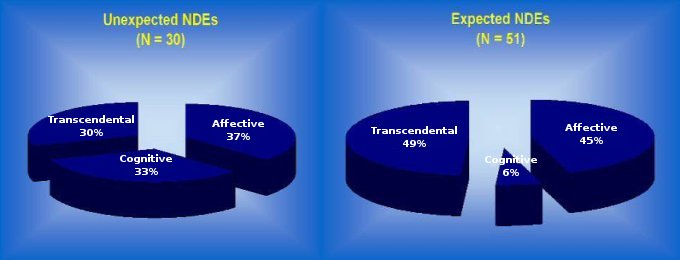
Greyson also found that NDEs due to expected life-threatening events mainly contain only affective and transcendental elements, while NDEs that result from unexpected life-threatening events are equally likely to contain cognitive, affective, and transcendental elements (Greyson 1985). (See Figure 1.) In other words, the expectation of encountering a life-threatening event modifies the content of an NDE, which is not what one would expect of a genuine afterlife experience that is the same for all people.
Other researchers have also uncovered evidence that the mere belief that one has died also determines NDE content (Gabbard, Twemlow, and Jones 1981; Owens, Cook, and Stevenson 1990). Yet none of these studies clearly differentiates between experiences and perceptions resulting from the causes of an NDE, and the features of the NDE itself. How can these be differentiated?
The Golden Gate Bridge and Skydiving
One way to identify the features endemic to the NDE itself is to examine the experiences of individuals who were never medically close to death when their NDEs occurred. Why do some people have NDEs under these circumstances, while others do not? One way to answer this question is to compare the experiences of those who survived jumping from the Golden Gate Bridge against the experiences of skydivers. From its completion in 1937 up until 2003, more than 1200 people have jumped from the Golden Gate Bridge in order to commit suicide (Friend 2003). The distance from the road surface of the bridge to the water is about 220 feet (67 meters), and it takes about 4 seconds to fall this distance before impacting at about 129 miles per hour (207 kilometers per hour). At this speed impact with the water is similar to high-speed impact with a concrete wall, so the resulting injuries are dreadful and nearly always fatal. Golden Gate Bridge jumpers who survived did not die because they entered the water feet first, suffering broken ankles and other lower limb fractures. At the time of his study, psychiatrist David Rosen interviewed 7 of the 10 people then known to have survived jumps from either the Golden Gate Bridge or the San Francisco-Oakland Bay Bridge. The 7 persons interviewed were between 16 and 36 years old. Except for the various reasons that they attempted suicide, they were all in good health, and they all expected to die as a result of jumping from their bridge. Surviving jumpers reported undergoing the following experiences as they fell toward the water (Rosen 1975):
- Time seemed to slow down, for the fall was experienced as taking a long time for each of them.
- Feelings of peace and tranquility.
Unlike many NDE reports, none of the surviving jumpers reported darkness or tunnel experiences, entering a region of light, a life review, meeting deceased family members or other figures, or entering a transcendental world (Rosen 1975).
This brings us to a discussion of a very similar experience—skydiving. Before opening their parachutes to land safely on the ground, skydivers leap out of airplanes and free fall for thousands of feet at the same velocities as those jumping from the Golden Gate Bridge or San Francisco-Oakland Bay Bridge. Both jumpers and skydivers are healthy and young. Neither undergo oxygen starvation during their falls. The only difference between them is in their respective mental states. Those jumping off of bridges want to die, and expect to die as a result of their actions, while pleasure-seeking skydivers certainly do not want to die, nor expect to die as a result of their actions.
It is very likely, then, that surviving bridge-jumpers experienced the true basic elements of an NDE, while other elements usually attributed to NDEs are actually products of a physiological condition that often causes an NDE. This proposition is reinforced by a fascinating study of the worldwide causes of death published by Christopher J. L. Murray and Alan D. Lopez in 1997. Murray and Lopez studied the causes of death of the 50.5 million people who died throughout the world during the year 1990 (Murray and Lopez 1997). Death is an irreversible loss of consciousness that accompanies the failure of vital body functions such as breathing and heartbeat. But what causes this loss of consciousness?
Consciousness is only possible when the reticular formation in the brainstem and the centromedian nucleus of the thalamus function normally. Failure or destruction of these two small parts of the brain—particularly the centromedian nucleus (or “thalamic switch”)—always causes unconsciousness (Woerlee 2008, Ch. 6). Malfunction or destruction may be a result of mechanical or disease-induced injury, toxins, toxic concentrations of metabolites, or drugs. This basic understanding of the neurological substrate of consciousness is essential for investigating how cause of death influences the perceptions of those reporting NDEs.
In about 92% of the dying, terminal loss of consciousness results from progressively severe oxygen starvation—eventually causing the failure of thalamic and brainstem functions (Murray and Lopez 1997). A plethora of conditions cause death by this mechanism: heart disease; cardiac arrest; having been shot through the heart; lung diseases such as pneumonia, tuberculosis, lung cancer, and so on; cancers of all other types; blood poisoning; snakebites; bleeding and blood loss; septic shock; and so on (Woerlee 2005, Ch. 15). But those who lose consciousness due to any of these conditions first undergo variable periods of increasing brain and perceptual malfunction due to oxygen starvation. And because the structure and function of the human body is the same all over the world, oxygen starvation produces a consistent set of manifestations. These include absence of pain, feelings of serene calm, unconcern, a lack of desire to move, and an inability to move. A review of one’s life and out-of-body experiences (OBEs) may also be generated by epileptic activity in the brain, while increased pupil diameter gives rise to an experience of light. Oxygen starvation may also induce retinal malfunction manifesting as an experience of a tunnel or darkness (Woerlee 2008, pp. 68-70). And because severe oxygen starvation sufficient to cause these experiences also affects memory consolidation, many of those who undergo them do not remember them (Woerlee 2005, Chs. 16-17). Those who do not recall their experiences are similar to those who suddenly faint. (Fainting is a typical form of loss of consciousness due to oxygen starvation of the brain.) Many who recover consciousness after fainting simply do not remember, or even realize that they fainted.
But the cause of the terminal loss of consciousness accompanying death is different in the remaining approximately 8% of people. Their loss of consciousness may be due to the accumulation of the toxic products of metabolism, or to kidney and liver diseases, uncontrolled diabetes mellitus, heatstroke, excessive cooling of the body, drugs and medicines inducing unconsciousness, alcohol, bleeding in the brain, brain tumors, head injury, blows to the head, or having been shot in the head. Each of these has quite different effects upon brain functioning before the affected persons lose consciousness, and the experiences due to these causes are different than those arising as a result of oxygen starvation. For example, the distribution of blood flow to the retina may produce tunnel experiences in people with oxygen starvation, but loss of consciousness due to sleep-inducing drugs (such as fast-acting anesthetics) may produce the experience of falling into a dark pit. Rapidly working sleep-inducing drugs produce the latter experience by first causing a failure in the central parts of the retina where the concentration of receptors is highest, before ultimately causing the failure of the entire retina (Woerlee 2008, pp. 237-241). So before loss of consciousness, these people may experience an NDE in combination with other perceptions and experiences induced by the cause of death, or by the cause of loss of consciousness.
Finally—the True Near-Death Experience
This brief discussion reveals three things which have never been adequately investigated, and reveals the true nature of NDEs as experiences that fall along the same spectrum as other human experiences:
- A true near-death experience consists of no more than the cognitive experience of time expansion combined with the affective emotions of peace and tranquility. All of the other perceptions and experiences erroneously attributed to NDEs are actually products of the physiological condition accompanying the NDE. Oxygen starvation of the brain is the cause of the terminal loss of consciousness in about 92% of the dying, and perceptions and emotions induced by oxygen starvation are often confused with the components of the NDE itself. The remaining roughly 8% who lose consciousness may have experiences that have nothing to do with oxygen starvation, but which are the products of different situations or disorders that may accompany NDEs.
- Individuals do not have NDEs unless during their experiences they believe (rightly or wrongly) that they are dead, that death is imminent, or that they are in a life-threatening situation.
- The nature of one’s NDE is affected by a person’s expectations.
Religion, Culture, and Appearance
But the fascinating issues raised by our present state of knowledge about NDEs does not end here. Consider the fact that the NDEs reported by individuals from different cultures differ considerably (Osis and Haraldsson 1986; Pasricha and Stevenson 1986). These differences primarily concern which pantheons of religious figures are seen, and the relationships to the NDEr of the persons encountered during the experience.
Not surprisingly, when religious figures are reported, Hindus tend to see Hindu religious figures, while Christians tend to see Christian religious figures. Moreover, many of the NDErs who report such encounters never question the apparent identity of such transcendental religious figures. But if the NDE reveals an objective transcendental world where deceased souls share eternal life, why does it feature the parochial gods of particular religions? I call these gods parochial because they are limited to this planet, and because belief in them only has a history of about 5,000 years—which is a fairly miniscule period of time compared to eternity. Shall we posit an afterlife divided into separate compartments for Muslims, Christians, Hindus, and so on? Compared to the eternity for which people are dead, people are alive for an extremely short period of time. So why do NDErs only report seeing the geographically and temporally local pantheons of gods of the religions that they know, instead of being awed by the true grandeur of a glorious eternal afterlife? This question has hitherto never raised by NDE investigators.
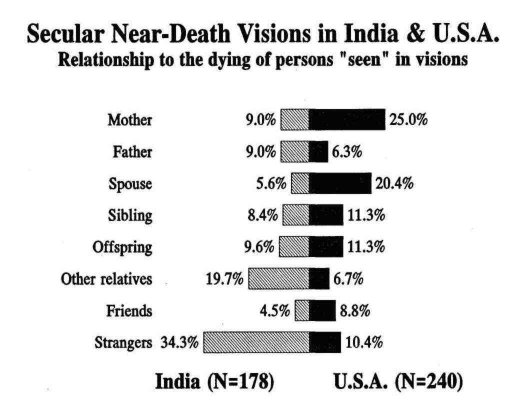
This brings us to the relationships of the other persons seen during NDEs to those reporting these experiences. Karlis Osis and Erlendur Haraldsson conducted a wonderful study of this issue among those from starkly different cultures (Osis and Haraldsson 1986). Unfortunately the study has not, to my knowledge, been replicated, but it is revealing and begs further investigation. At the time of the study medical practitioners recounting patients’ oral reports of deathbed visions in India recalled that their dying patients mainly reported apparitions of unidentified deceased persons and relatives who greeted them and guided them into the transcendental world of the dead. By contrast, the recounted reports of dying patients in the United States mainly featured apparitions of deceased spouses or mothers who performed the same functions (p < 0.001). (See Figure 2.) Does this mean that when a person from India dies, random souls are conscripted to guide that person into the afterlife, while a dying American is privileged to be guided by deceased mothers or spouses? This finding does not sit well with the idea of a shared afterlife which should largely be the same for all people. But the issue is never studied or even raised by current NDE researchers.
Scour the NDE reports from a variety a sources and a unified but surprising picture arises: deceased family members encountered in NDEs are nearly always described as vital and healthy versions of their formerly living selves, just as NDErs last remembered them! Does this mean that when an older man dies, he must spend eternity with the appearance of a vital senior citizen? I asked several men and women how they would like to appear throughout an eternal afterlife. Not surprisingly, all of them vehemently rejected the idea of spending eternity with an older appearance, no matter how vital. If you asked older persons how they would like to appear, they too would probably want to appear as young and vital. So if the transcendental world seen during NDEs truly represents a shared afterlife, why those who died in their golden years appear older during NDE encounters? This is another fascinating question that is never even raised by near-death researchers.
The Immaterial Soul
OBEs occur quite frequently during NDEs, and are often taken to be irrefutable proof for the reality of an immaterial soul. I will not summarize the extensive studies that have been done on OBEs, but instead will highlight an aspect of this fascinating experience that never seems to be mentioned by those who study this phenomenon. Individuals often report that during their OBEs they actually saw people, events, and objects, and heard sounds and speech. Many of their visual and auditory perceptions are even subsequently confirmed. Those who believe that OBEs are experiences of a disembodied consciousness always refer to these veridical observations as the ultimate confirmation of their beliefs. However, these observations confirm quite the opposite.
Those who report OBEs say that their out-of-body form is invisible and immaterial. Invisibility is inferred by the fact that other people never report seeing their disembodied selves, and that no-one has ever photographed such a disembodied consciousness. Their immateriality is inferred from their reported ability to pass through their own bodies, doors, brick walls, and roofs, as if these things presented no barrier to their ostensibly disembodied selves. Taken literally, all of this implies that an invisible and immaterial disembodied consciousness does not interact with physical forces like electromagnetic radiation (such as visible light), or with matter (including sound waves in air). This absence of interaction with physical matter and forces implies that a disembodied consciousness cannot see or hear during an OBE. So how could the disembodied consciousness of a person see and hear during an OBE? (See extensive discussions on this in Woerlee 2008, pp. 120-123 and 264-266.) No one has really attempted to answer this question. People—including near-death researchers—generally just accept the notion of out-of-body vision and hearing at face value without further reflection about what it would take to make it possible.
Conclusions
Current knowledge and studies of the NDE phenomenon reveal fascinating inconsistencies and several poorly researched questions. Further study is necessary to elucidate the points raised in this article so as to dispel the aura of popular New Age mysticism surrounding the NDE. Given the nature of the questions raised, it is quite likely that the only logical conclusion that such studies could support would be that the NDE is a no more than a profound hallucinatory experience undergone by those who perceive themselves to be dead, or in a life-threatening situation, at the time of the NDE. Nonetheless, despite its hallucinatory nature, the NDE does reveal the deepest reaches of the individual psyche, as well as the sociocultural influences upon the individual psyche. It is also an experience that has profound effects upon the individuals that undergo it. All of these points provide very good reasons to learn more about the true nature of the NDE.
References
Beauregard, Mario and Denyse O’Leary. The Spiritual Brain: A Neuroscientist’s Case for the Existence of the Soul. New York, NY: Harper Collins, 2007.
Evans-Wentz, Walter Y. (trans.) The Tibetan Book of the Dead. London, UK: Oxford University Press, 1960.
Friend, Tad. “Jumpers: The Fatal Grandeur of the Golden Gate Bridge.” The New Yorker. October 13, 2003.
Gabbard, Glen O., Stuart W. Twemlow, and Fowler C. Jones. “Do ‘Near-Death Experiences’ Occur Only Near Death?” Journal of Nervous and Mental Disease. Vol. 169, No. 6 (June 1981): 374-377.
Grey, Margot. Return from Death: An Exploration of the Near-Death Experience. London, UK: Arkana, 1986.
Greyson, Bruce. “Incidence and Correlates of Near-Death Experiences in a Cardiac Care Unit.” General Hospital Psychiatry. Vol. 25, No. 4 (July/August 2003): 269-276.
Greyson, Bruce. “The Near-Death Experience Scale: Construction, Reliability, and Validity. Journal of Nervous and Mental Disease. Vol. 171, No. 6 (June 1983): 369-375.
Greyson, Bruce. “A Typology of Near-Death Experiences.” American Journal of Psychiatry. Vol. 142, No. 8 (August 1985): 967-969.
Lange, Rense, Bruce Greyson, and James Houran. “A Rasch Scaling Validation of a ‘Core’ Near-Death Experience.” British Journal of Psychology. Vol. 95, Pt. 2 (May 2004): 161-177.
Lempert, T., M. Bauer, and D. Schmidt. “Syncope: A Videometric Analysis of 56 Episodes of Transient Cerebral Hypoxia.” Annals of Neurology. Vol. 35, No. 2 (August 1994): 233-237.
Moody, Raymond. Life After Life: The Investigation of a Phenomenon—Survival of Bodily Death. Covington, CA: Mockingbird Books, 1975.
Murray, Christopher J. L. and Alan D. Lopez. “Mortality by Cause for Eight Regions of the World: Global Burden of Disease Study.” Lancet. Vol. 349, Issue 9061 (May 3, 1997): 1269-1276.
Osis, Karlis and Erlendur Haraldsson. At the Hour of Death: The Results of Research on Over 1000 Afterlife Experiences. New York, NY: Avon Books, 1977.
Owens, Justine E., Emily Williams Cook, and Ian Stevenson. “Features of ‘Near-Death Experience’ in Relation to Whether or Not Patients were Near Death.” Lancet. Vol. 336, Issue 8724 (November 10, 1990): 1175-1177.
Parnia, Sam, D. G. Waller, R. Yeates, and Peter Fenwick. “A Qualitative and Quantitative Study of the Incidence, Features and Aetiology of Near Death Experiences in Cardiac Arrest Survivors.” Resuscitation. Vol. 48, No. 2 (February 2001): 149-156.
Pasricha, Satwant and Ian Stevenson. “Near-Death Experiences in India: A Preliminary Report.” Journal of Nervous and Mental Disease. Vol. 174, No. 3 (March 1986): 165-174.
Rawlings, Maurice. Beyond Death’s Door. New York, NY: Bantam Books, 1979.
Ring, Kenneth. Life at Death: A Scientific Investigation of the Near-Death Experience. New York: Coward, McCann & Geoghegan, 1980.
Rosen, David H. “Suicide Survivors: A Follow-Up Study of Persons Who Survived Jumping from the Golden Gate and San Francisco-Oakland Bay Bridges.” Western Journal of Medicine. Vol. 122, No. 4 (April 1975): 289-294.
Sabom, Michael B. Recollections of Death: A Medical Investigation. New York, NY: Harper & Row, 1982.
van Lommel, Pim. Eindeloos Bewustzijn: Een Wetenschappelijke Visie Op De Bijna-Doodervaring. Kampen, The Netherlands: Ten Have, 2007.
van Lommel, Pim, Ruud van Wees, Vincent Meyers, and Ingrid Elfferich. “Near-Death Experiences in Survivors of Cardiac Arrest: A Prospective Study in the Netherlands.” Lancet. Vol. 358, Issue 9298 (December 15, 2001): 2039-2045.
Woerlee, G. M. Mortal Minds: The Biology of Near Death Experiences. Amherst, NY: Prometheus Books, 2005.
Woerlee, G. M. The Unholy Legacy of Abraham. Bangor, ME: BookLocker, 2008. Companion website: <http://www.unholylegacy.woerlee.org>
Copyright ©2009 Gerald M. Woerlee. The electronic version is copyright ©2009 by Internet Infidels, Inc. with the written permission of Gerald M. Woerlee. All rights reserved.